

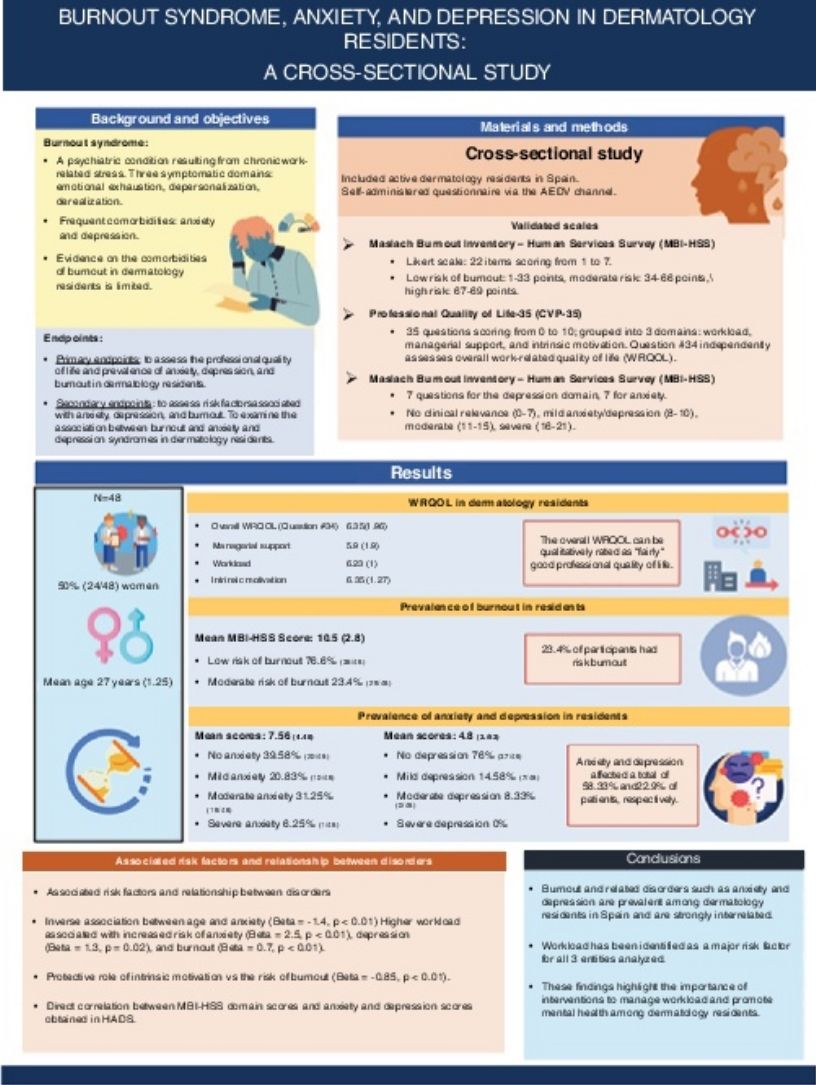
Burnout syndrome is a mental health disorder due to chronic occupational stress. Both burnout and associated comorbidities are prevalent among health care professionals, being medical residents a vulnerable group. Despite this, the scientific medical literature currently available on this issue in dermatology residents is scarce. The aim of this study was to analyze the prevalence of the burnout syndrome, anxiety, and depression in dermatology residents, and the associated risk factors.
Material and MethodThis was a cross-sectional trial designed to include dermatology residents from Spain (from December 2022 through June 2023). A self-administered form was sent via online messaging applications, including validated scales to study professional quality of life, burnout syndrome, anxiety, and depression.
ResultsA total of 48 dermatology residents were included in the study, 50% of whom (24/48) were women, with a mean age of 27 years (1.25). A total of 58.33% (28/48) of the residents had some degree of anxiety, 22.9% (11/48) some degree of depression, and 23.4% a moderate risk of burnout (11/48). Workload was the main risk factor associated with the 3 disorders studied, while managerial support or intrinsic motivation seem to play a protective role.
ConclusionsBurnout syndrome and its comorbidities are both prevalent in dermatology residents in Spain and closely related to each other.
El síndrome de burnout es un trastorno de salud mental derivado del estrés laboral crónico. Tanto el burnout como las comorbilidades asociadas son prevalentes en profesionales sanitarios, siendo los médicos residentes un grupo vulnerable. Pese a ello, la literatura que analiza este tema en residentes de dermatología es escasa. El presente estudio tiene como objetivo analizar las prevalencias de burnout, ansiedad y depresión en residentes de dermatología, así como los factores de riesgo asociados.
Material y métodoSe diseñó un estudio transversal que incluyó residentes de dermatología en España (diciembre de 2022 a junio de 2023). Se empleó un formulario autoadministrado, enviado mediante aplicaciones de mensajería online, en el cual se incluyeron las escalas validadas para el análisis de la calidad de vida profesional, el síndrome de burnout, la ansiedad y la depresión.
ResultadosUn total de 48 residentes de dermatología fueron incluidos en el estudio, siendo el 50% (24/48) mujeres, y la edad media de 27 (1,25) años. El 58,33% (28/48) de los residentes presentó ansiedad de algún grado, el 22,9% (11/48) manifestó algún grado de depresión y el 23,4% presentó riesgo moderado de padecer burnout (11/48). La carga de trabajo fue el principal factor de riesgo asociado a los 3 trastornos estudiados, mientras que el apoyo de los directivos o la motivación intrínseca parecen jugar un papel protector.
ConclusionesEl síndrome de burnout y sus comorbilidades son prevalentes en residentes de dermatología en España y están estrechamente relacionados entre sí.

Burnout syndrome or professional exhaustion syndrome is a psychiatric disorder derived from chronic work-related stress, characterized by 3 major symptom domains: emotional exhaustion, depersonalization, and derealization.1–3 The high prevalence of this syndrome among health care professionals has sparked interest in investigating the main factors associated with it, such as excessive administrative work, excessive computerization, or low remuneration.2,4 Furthermore, not all professional categories appear to be equally vulnerable: some studies show a higher risk of burnout in residents vs other categories.5–7 Among the risk factors described for developinh burnout in residents, excessive workload and lack of free time to the detriment of study hours have been reported.8,9
All the above-mentioned described risk factors are framed within a concept: professional quality of life (PQoL), which could be defined as the balance between work demands and the ability to meet the needs of other areas of life,10 a balance that, if disrupted toward work-related stress, would easily lead to burnout syndrome.5,11
Although the available literature on burnout in the medical field has been growing, most researches approach this syndrome as an outcome variable, without evaluating its association with other psychiatric comorbidities, such as anxiety or depression.12 These entities often coexist, potentially feeding into each other and aggravating the symptoms.12,13 A harmful work environment and occupational stress, classically related to burnout, may act by inducing or aggravating mental health disorders such as anxiety and depression, in a continuum in which burnout syndrome appears to mediate,13,14 while at the same time, these psychiatric conditions are considered independent clinical entities by the 11th version of the International Classification of Diseases.15
Against some predictions, dermatology has shown not to be free from the threat of burnout,4,16 and requires deeper studies into the main risk factors identified in the working environment, as well as studies analyzing the psychiatric comorbidity associated with burnout in dermatologists and a specific analysis of the prevalence of professional exhaustion in the highest-risk category within medical practice: residents.8,17
Given the absence of studies in our environment on these issues, we designed cross-sectional study to identify the prevalence of burnout among Spanish dermatology residents, the associated risk factors, and its association with anxiety and depression.
Materials and methodsDesignWe designed a cross-sectional study, including doctors currently undergoing dermatology residency in Spain, to whom a self-administered form was sent via online instant messaging applications (internal communication service of the Spanish Academy of Dermatology and Venereology) from December 2022 through June 2023.
EndpointsPrimary endpoints were to assess the professional quality of life and prevalence of anxiety, depression, and burnout among dermatology residents.
Secondary endpoints were to analyze the risk factors associated with anxiety, depression, and burnout, and assess the association between burnout and anxiety and depression syndromes in dermatology residents.
Inclusion and exclusion criteriaInclusion criteria were being a dermatology resident and practicing in Spain during the study period.
Exclusion criteria were refusal to participate in the study, submission of the questionnaire more than once, or incomplete submission.
Measurement instrumentsThe self-administered form includes several sociodemographic and work-related variables, as well as validated scales for the evaluation and diagnosis of the variables of interest.
To evaluate PQoL, the Professional Quality of Life-35 (PQoL-35) questionnaire was used, validated in Spanish for its application to physicians—residents included—and for online administration purposes.18,19 The PQoL-35 scale evaluates PQoL across 35 questions rated from 0 to 10, grouped into 3 domains: workload, managerial support, and intrinsic motivation. Question #34 is an independent question assessing overall work-life quality. The score given to each question can be classified as follows: “nothing” (values 1 and 2), “somewhat” (values 3, 4, and 5), “quite a lot” (values 6, 7, and 8), and “very much” (values 9 and 10).
To evaluate burnout and its different domains, the Maslach Burnout Inventory-Human Services Survey (MBI-HSS) was used, also validated for use in Spanish and physicians.20 The MBI-HSS consists of 22 items using a 7-point Likert scale where a response of 1 indicates no disorder and a score of 7 indicates the maximum intensity of burnout symptoms. The different questions are structured within the domains of emotional exhaustion, depersonalization, and derealization. MBI-HSS scores are considered low between 1 and 33, medium between 34 and 66, and high between 67 and 69. Although there are no actual cutoff scores, it is also accepted that high scores in emotional exhaustion (≥ 26) and depersonalization (≥ 9) and low in derealization (≤ 34) define burnout.
Anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale (HADS), which has a validated version in Spanish.21 The HADS scale comprises 17 Likert-type questions that progressively assess symptom intensity, with scores ranging from 0 to 3. Seven of these questions evaluate the presence of anxiety, and 7 the presence of depression. The sum of the scores obtained is interpreted as follows: no clinical relevance (0–7), mild anxiety/depression (8–10), moderate anxiety/depression (11–15), severe anxiety/depression (16–21).
Statistical analysisDescriptive statistics were used to evaluate the characteristics of the sample. The Shapiro-Wilk test was used to assess the normality of the variables. Continuous variables were expressed as mean and standard deviation, and qualitative ones as distributions of relative and absolute frequencies. The chi-square test or Fisher's exact test, as appropriate, was used to compare nominal variables, while the Student's t-test, or Wilcoxon-Mann-Whitney test were used to make comparisons between nominal and continuous data. In case of multiple comparisons, a first association analysis was performed using ANOVA, with a subsequent post-hoc correction using Tukey's HSD statistic in case of statistical significance. To explore possible associated factors, simple linear regression was used for continuous variables. The Beta coefficient and standard deviation were used to predict the logarithmic probabilities of the dependent variable. Statistical significance was considered if p-values were <0.05. Statistical analyses were performed using JMP version 14.1.0 (SAS Institute, Cary, NC, United States).
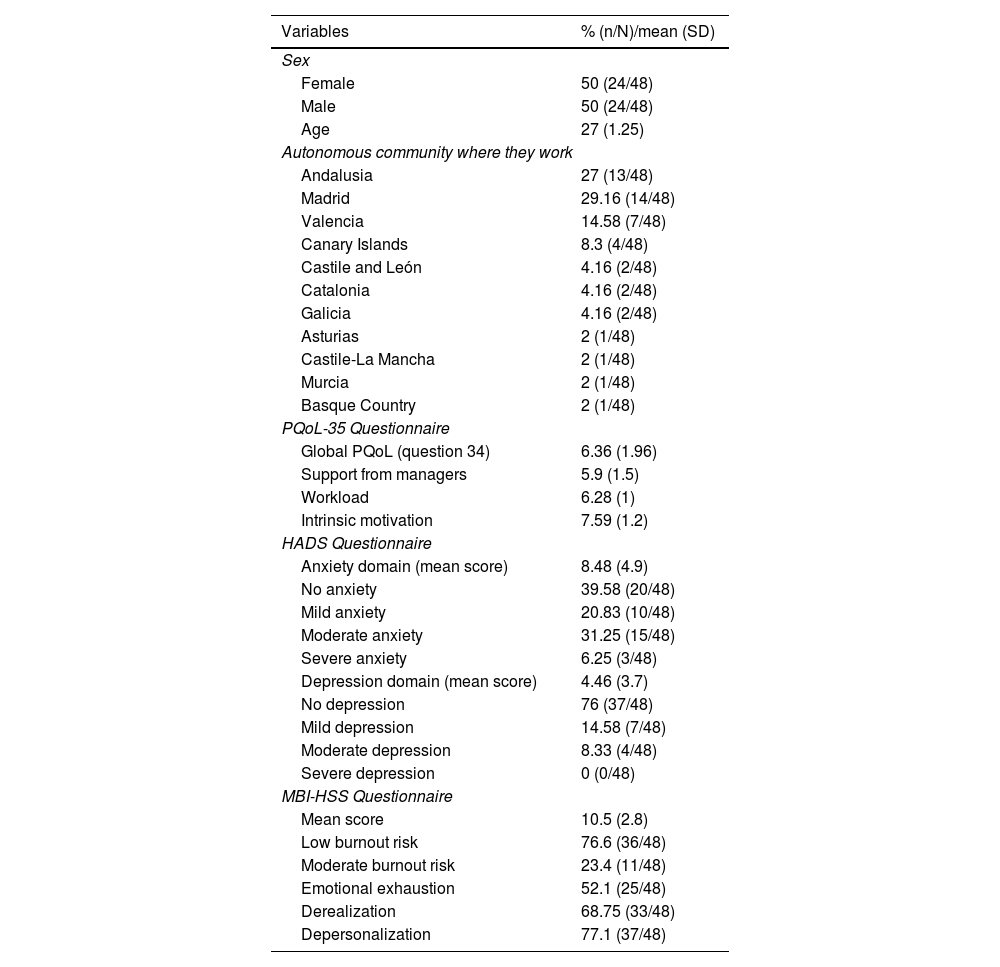
ResultsDescriptive study of the sampleA total of 48 dermatology residents were included in the study, with 50% (24/48) being women, and a mean age of 27 (1.25) years. A total of 54.16% of participants were in their second year of residency (26/48) (Table 1).
Descriptive study of the sample.
| Variables | % (n/N)/mean (SD) |
|---|---|
| Sex | |
| Female | 50 (24/48) |
| Male | 50 (24/48) |
| Age | 27 (1.25) |
| Autonomous community where they work | |
| Andalusia | 27 (13/48) |
| Madrid | 29.16 (14/48) |
| Valencia | 14.58 (7/48) |
| Canary Islands | 8.3 (4/48) |
| Castile and León | 4.16 (2/48) |
| Catalonia | 4.16 (2/48) |
| Galicia | 4.16 (2/48) |
| Asturias | 2 (1/48) |
| Castile-La Mancha | 2 (1/48) |
| Murcia | 2 (1/48) |
| Basque Country | 2 (1/48) |
| PQoL-35 Questionnaire | |
| Global PQoL (question 34) | 6.36 (1.96) |
| Support from managers | 5.9 (1.5) |
| Workload | 6.28 (1) |
| Intrinsic motivation | 7.59 (1.2) |
| HADS Questionnaire | |
| Anxiety domain (mean score) | 8.48 (4.9) |
| No anxiety | 39.58 (20/48) |
| Mild anxiety | 20.83 (10/48) |
| Moderate anxiety | 31.25 (15/48) |
| Severe anxiety | 6.25 (3/48) |
| Depression domain (mean score) | 4.46 (3.7) |
| No depression | 76 (37/48) |
| Mild depression | 14.58 (7/48) |
| Moderate depression | 8.33 (4/48) |
| Severe depression | 0 (0/48) |
| MBI-HSS Questionnaire | |
| Mean score | 10.5 (2.8) |
| Low burnout risk | 76.6 (36/48) |
| Moderate burnout risk | 23.4 (11/48) |
| Emotional exhaustion | 52.1 (25/48) |
| Derealization | 68.75 (33/48) |
| Depersonalization | 77.1 (37/48) |
PQoL-35: Professional Quality of Life-35; SD: standard deviation; HADS: Hospital Anxiety and Depression Scale; MBI-HSS: Maslach Burnout Inventory-Human Services Survey.
Overall work-life quality obtained a mean score of 6.36 (1.96). For each domain of the PQoL-35 scale, the scores were: managerial support, 5.91 (1.4, “somewhat” supportive); workload, 6.28 (1.2, “quite a lot” of workload); and intrinsic motivation, 7.59 (1.2, “quite a lot” of motivation).
Regarding the anxiety domain of HADS, the mean score was 8.5 (4.9); 58.33% (28/48) of participants had some degree of anxiety; 20.83%, mild anxiety (10/48); 31.25%, moderate anxiety (15/48); and 6.25%, severe anxiety (3/48). Depression had a mean score of 4.46 (3.7) and was present in 22.9% (11/48) of residents; 14.58% (7/48) exhibited mild depression and 8.33% (4/48), moderate depression.
Burnout syndrome, assessed using the MBI-HSS, obtained a global score of 10.5 (2.8). A total of 23.4% of the residents had a moderate risk of burnout (11/48), while the rest were categorized as low-risk residents.
The remaining descriptive study variables are shown in Table 1.
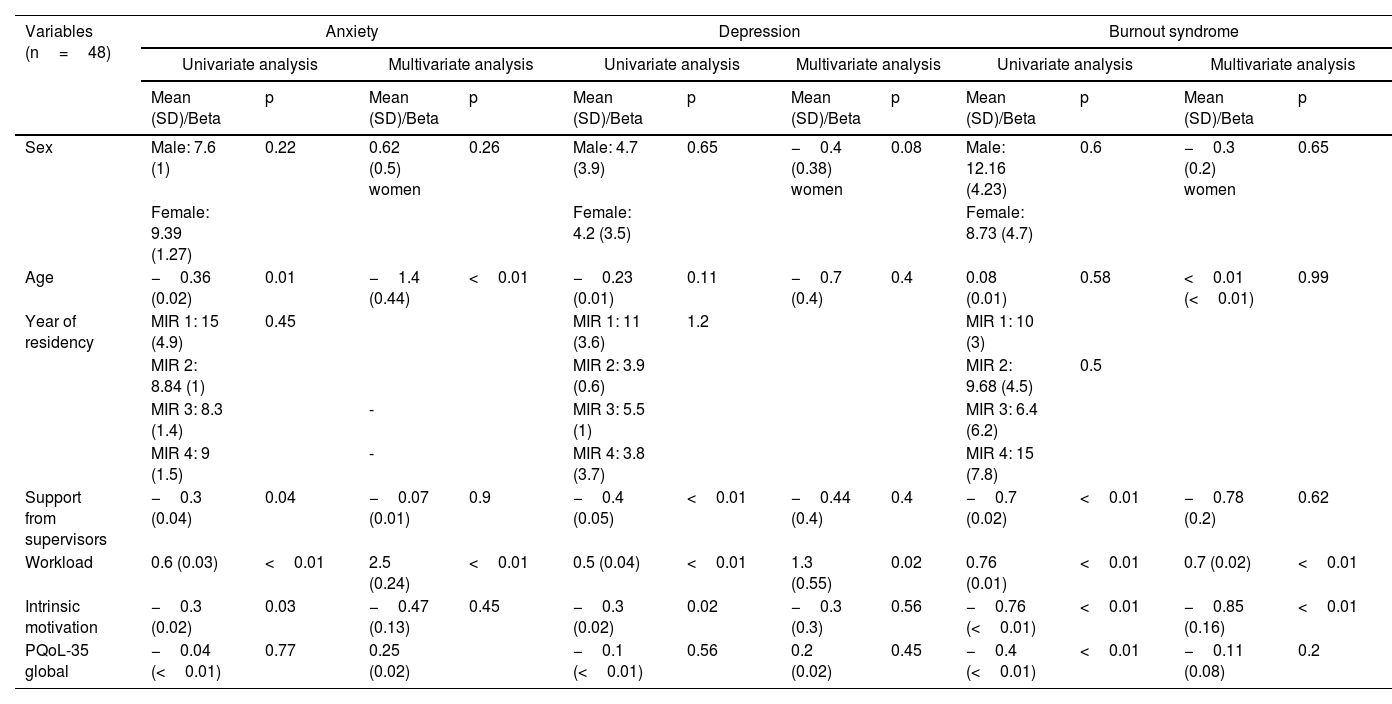
Risk factors for anxiety in dermatology residentsA statistically significant negative correlation with age was found, which remained independent in the multivariable analysis (Beta=−1.4; p<0.01). Other sociodemographic variables, such as sex or the residency year did not show an association with anxiety.
Regarding PQoL, a higher workload was associated with a greater risk of anxiety in the multivariable analysis (Beta=2.5; p<0.01). Although managerial support and intrinsic motivation showed an inverse association with anxiety in the univariate analysis, they did not remain independent.
Risk factors for depression in dermatology residentsNo sociodemographic variables were identified as associated with a higher risk of depression in the sample. However, regarding PQoL, an independent positive correlation was found between workload and the depression score on the HADS scale (Beta=1.3; p=0.02).
An inverse correlation between the risk of depression and the domains of managerial support and intrinsic motivation was described in the univariate analysis.
Risk factors for burnout in dermatology residentsNo sociodemographic risk factors for burnout syndrome were identified in the study. Workload was independently associated with the risk of burnout in the multivariable analysis (Beta=0.7; p<0.01), while managerial support was found to be inversely associated with the MBI-HSS score in the same analysis (Beta=−0.85; p<0.01). Intrinsic motivation was described as inversely associated with the MBI-HSS score in the univariate analysis (Table 2)
Sociodemographic and professional quality of life factors associated with burnout, anxiety, and depression: univariate and multivariate analyses.
| Variables (n=48) | Anxiety | Depression | Burnout syndrome | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate analysis | Multivariate analysis | Univariate analysis | Multivariate analysis | Univariate analysis | Multivariate analysis | |||||||
| Mean (SD)/Beta | p | Mean (SD)/Beta | p | Mean (SD)/Beta | p | Mean (SD)/Beta | p | Mean (SD)/Beta | p | Mean (SD)/Beta | p | |
| Sex | Male: 7.6 (1) | 0.22 | 0.62 (0.5) women | 0.26 | Male: 4.7 (3.9) | 0.65 | −0.4 (0.38) women | 0.08 | Male: 12.16 (4.23) | 0.6 | −0.3 (0.2) women | 0.65 |
| Female: 9.39 (1.27) | Female: 4.2 (3.5) | Female: 8.73 (4.7) | ||||||||||
| Age | −0.36 (0.02) | 0.01 | −1.4 (0.44) | <0.01 | −0.23 (0.01) | 0.11 | −0.7 (0.4) | 0.4 | 0.08 (0.01) | 0.58 | <0.01 (<0.01) | 0.99 |
| Year of residency | MIR 1: 15 (4.9) | 0.45 | MIR 1: 11 (3.6) | 1.2 | MIR 1: 10 (3) | |||||||
| MIR 2: 8.84 (1) | MIR 2: 3.9 (0.6) | MIR 2: 9.68 (4.5) | 0.5 | |||||||||
| MIR 3: 8.3 (1.4) | - | MIR 3: 5.5 (1) | MIR 3: 6.4 (6.2) | |||||||||
| MIR 4: 9 (1.5) | - | MIR 4: 3.8 (3.7) | MIR 4: 15 (7.8) | |||||||||
| Support from supervisors | −0.3 (0.04) | 0.04 | −0.07 (0.01) | 0.9 | −0.4 (0.05) | <0.01 | −0.44 (0.4) | 0.4 | −0.7 (0.02) | <0.01 | −0.78 (0.2) | 0.62 |
| Workload | 0.6 (0.03) | <0.01 | 2.5 (0.24) | <0.01 | 0.5 (0.04) | <0.01 | 1.3 (0.55) | 0.02 | 0.76 (0.01) | <0.01 | 0.7 (0.02) | <0.01 |
| Intrinsic motivation | −0.3 (0.02) | 0.03 | −0.47 (0.13) | 0.45 | −0.3 (0.02) | 0.02 | −0.3 (0.3) | 0.56 | −0.76 (<0.01) | <0.01 | −0.85 (0.16) | <0.01 |
| PQoL-35 global | −0.04 (<0.01) | 0.77 | 0.25 (0.02) | −0.1 (<0.01) | 0.56 | 0.2 (0.02) | 0.45 | −0.4 (<0.01) | <0.01 | −0.11 (0.08) | 0.2 | |
PQoL-35, professional quality of life; SD, standard deviation; MIR, internal resident medical physician.
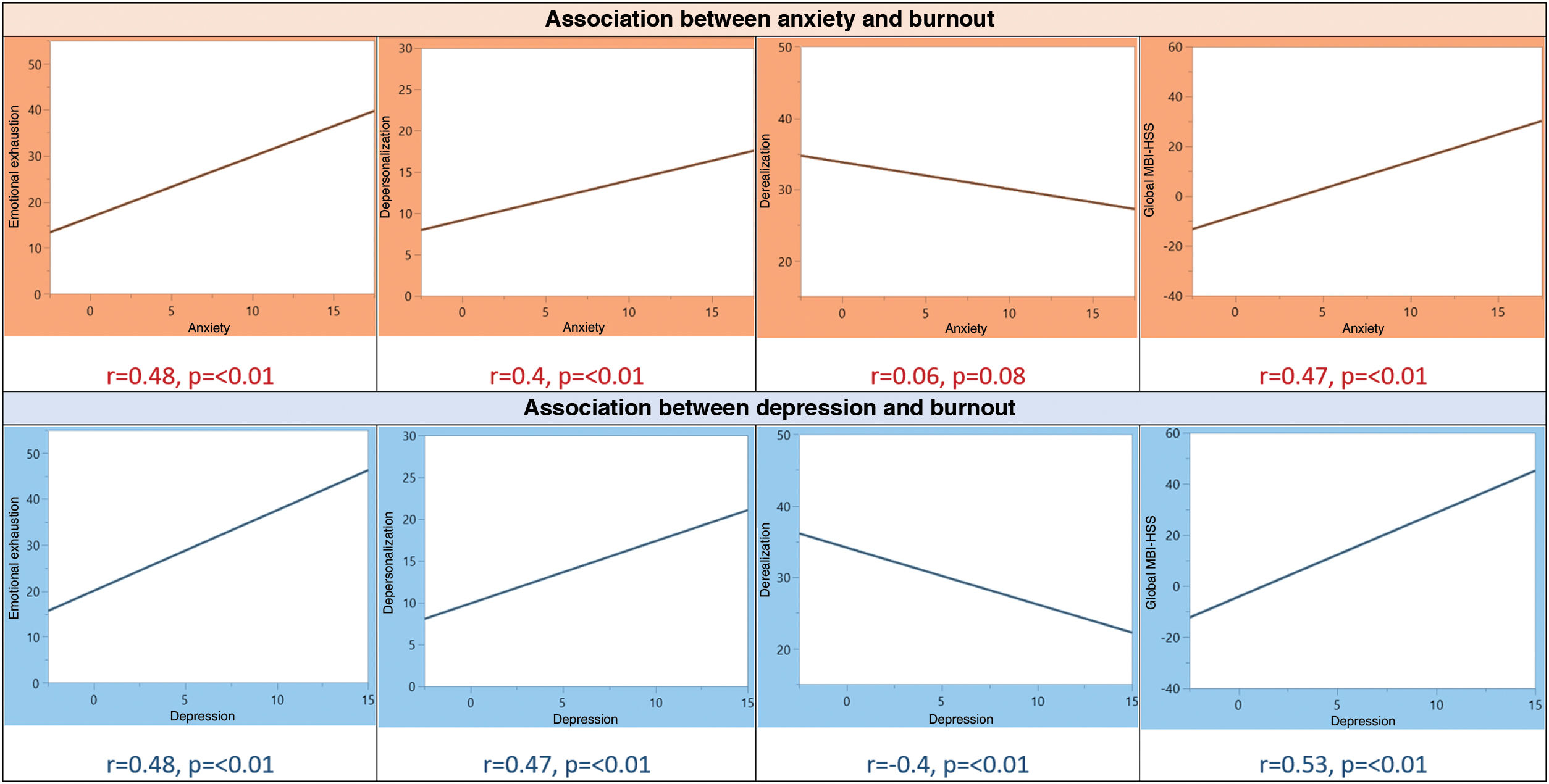
To interpret these results, it should be noted that the derealization domain in the MBI-HSS is scored inversely to the others: a negative r between derealization and another variable should be interpreted as a direct correlation.
The score obtained on the HADS scale for anxiety symptoms showed a direct correlation with the domains of emotional exhaustion (r=0.48; p<0.01) and depersonalization (r=0.4; p<0.01), with no association ever found with the derealization domain. Similarly, a statistically significant positive association was observed between depression and the domains of emotional exhaustion (r=0.48; p<0.01), depersonalization (r=0.47; p<0.01), and burnout derealization (r=−0.4; p<0.01). Higher global scores on the MBI-HSS were associated with a greater risk of anxiety (r=0.47; p<0.01) and depression (r=0.53; p<0.01) (Figure 1).
Discussion
The present cross-sectional study analyzed the prevalence and associated risk factors for burnout syndrome and other related mental health disorders in 48 dermatology residents. Although based on the study results, 58.33% (28/48) of participants presented with some degree of anxiety, 22.9% (11/48) of the surveyed residents reported some degree of depression, and 23.4% showed a moderate risk of burnout (11/48), more than half of the participants experienced some symptoms of burnout. The sociodemographic characteristics of the sample are similar to those obtained in studies on the same topic.8,22
The burnout prevalences identified in this study are similar, albeit lower, to those observed in a systematic review and meta-analysis of 26 articles that included residents from different medical specialties.9 Unfortunately, dermatology residents were not included, and the prevalences found varied significantly depending on the medical specialties.9 A prevalence study conducted among French dermatologists (residents and licensed specialists) shows similar results of moderate burnout risk (15.6%)23; similarly, a cross-sectional design in Egyptian dermatologists also showed that more than half of the participants presented with, at least, 1 burnout symptom, and that residents had more chances of experiencing additional psychiatric comorbidities.24 Regarding specific studies in dermatology residents, we find results consistent with those provided by a Canadian study of 116 dermatology residents, where more than half of the participants showed depersonalization or affective exhaustion, and around 40% exhibited symptoms of derealization.8 The prevalences of anxiety and depression described in our study are similar to those obtained in cross-sectional studies conducted among psychiatry and family medicine residents25,26; however, the prevalences of depression found in cross-sectional studies of dermatology residents are higher than those described in our sample.8 It is difficult to clarify these differences due to the use of different diagnostic tools.8
Workload was directly correlated with a higher risk of anxiety and depression in residents, independently of other variables. On the contrary, greater managerial support and higher intrinsic motivation appeared to play a protective role, although this could not be demonstrated in the multivariable analysis. In this regard, a cross-sectional study of 116 dermatology residents reflects a significant number of hours devoted to study and work and highlights managerial support as a protective factor against burnout in residents.8 The role of workload as a risk factor in psychiatric entities other than burnout lends credence to the potential relationship between these disorders and the theory that chronic work stress can have an impact beyond the purely work-related sphere.12
Older age implied a lower risk of anxiety in dermatology residents, an association that remained significant in the multivariable analysis. This protective role has been described in other studies and could be explained by the development of greater resilience, greater job satisfaction, or the acquisition of self-care tools.27,28
Similarly, although workload was associated with a higher risk of burnout regardless of other variables, intrinsic motivation showed an inverse correlation (a protective role). These results are consistent with other studies, where elements related to workload, such as excessive bureaucratization and lack of free time, have been identified as risk factors for the burnout syndrome.4,7,8 Self-care and enhancing personal motivation have been proposed as measures to prevent burnout among dermatologists,4,17 reinforcing the protective role that intrinsic motivation has shown in this work.
In this study, a direct correlation was identified between most burnout domains and the intensity of anxiety and depression symptoms. The relationship between burnout and other psychiatric conditions among physicians has been demonstrated in other studies.8,12,29 A systematic review of cross-sectional studies identified 12 studies that analyzed the relationship between burnout and anxiety, finding a significant association with similar correlations to those obtained in our study.12 In general, 45 of the 61 studies from a systematic review that analyzed the relationship between burnout and depression reported a statistically significant association, especially with the domain of emotional exhaustion,12 which was the domain most strongly correlated with depression in our work.
It is essential to pay attention to the mental health issues affecting dermatologists in the workplace. On the one hand, burnout prevention programs can focus on modifying the risk factors present in the work environment. Work overload, excessive bureaucratization, and lack of free time have been identified as risk factors for developing the burnout syndrome.4,14 On the other hand, it is crucial to foster tools that individuals themselves can develop to prevent mental health problems in the work environment. Measures such as recognizing symptoms, self-care, and promoting personal motivation have been recommended to prevent burnout in dermatologists.4,17
ConclusionsThis study shows, for the first time, the state of professional quality of life among dermatology residents in Spain, the prevalence of mental health disorders related to chronic work stress, and the risk factors involved. However, there are limitations: the sample size is small, and the cross-sectional design of the study makes it impossible to find causal associations. Additionally, the use of a self-administered form—despite using validated scales—may have been a source of selection bias in the sample, potentially facilitating the participation of residents with a higher risk of burnout than that found in the overall study population. On the other hand, the response rate obtained was low: if we consider that approximately 420 dermatology residents currently active in Spain are academic members of the Spanish Academy of Dermatology and Venereology and, therefore, had access to the form, the response rate would be 11.43%.
Based on our results, the burnout syndrome and related disorders, such as anxiety and depression, are prevalent among dermatology residents in Spain and are strongly related to each other. Workload has been identified as the main risk factor for all 3 entities analyzed, while managerial support and intrinsic motivation appear to play a protective role. These findings highlight how important interventions are for managing workload and promoting mental health among dermatology residents.
Conflicts of interestNone declared.



