



Idiopathic facial aseptic granuloma (IFAG) is a pediatric condition first described in 1999 by a group of French dermatologists who used the name pyodermite froide because of the lesion's resemblance to an abscess, although with mild signs of inflammation.1,2 The condition is characterized by the appearance of 1 or more painless red to violaceous nodules on the face, typically located on the cheeks or eyelids.1 The lesions are benign, last from a few months to a year, and usually heal without leaving a scar.2
Histologic examination reveals a granulomatous inflammatory response similar to that observed in granulomas caused by foreign bodies or infectious agents such as mycobacteria.2 Ultrasound studies reveal a solid hypoechoic lesion without calcium deposits.3
We present the case of a 2-year-old girl with no past medical history of interest who was referred to our clinic because of an asymptomatic nodular lesion on the left cheek that had appeared approximately 2 months before the consultation (Fig. 1). Physical examination revealed a red to violaceous nodule of approximately 1cm in diameter; the painless lesion was nonfluctuant on palpation and no regional lymph node involvement was observed. When questioned, the infant ‘s mother did not recall any insect bite or trauma at the site.

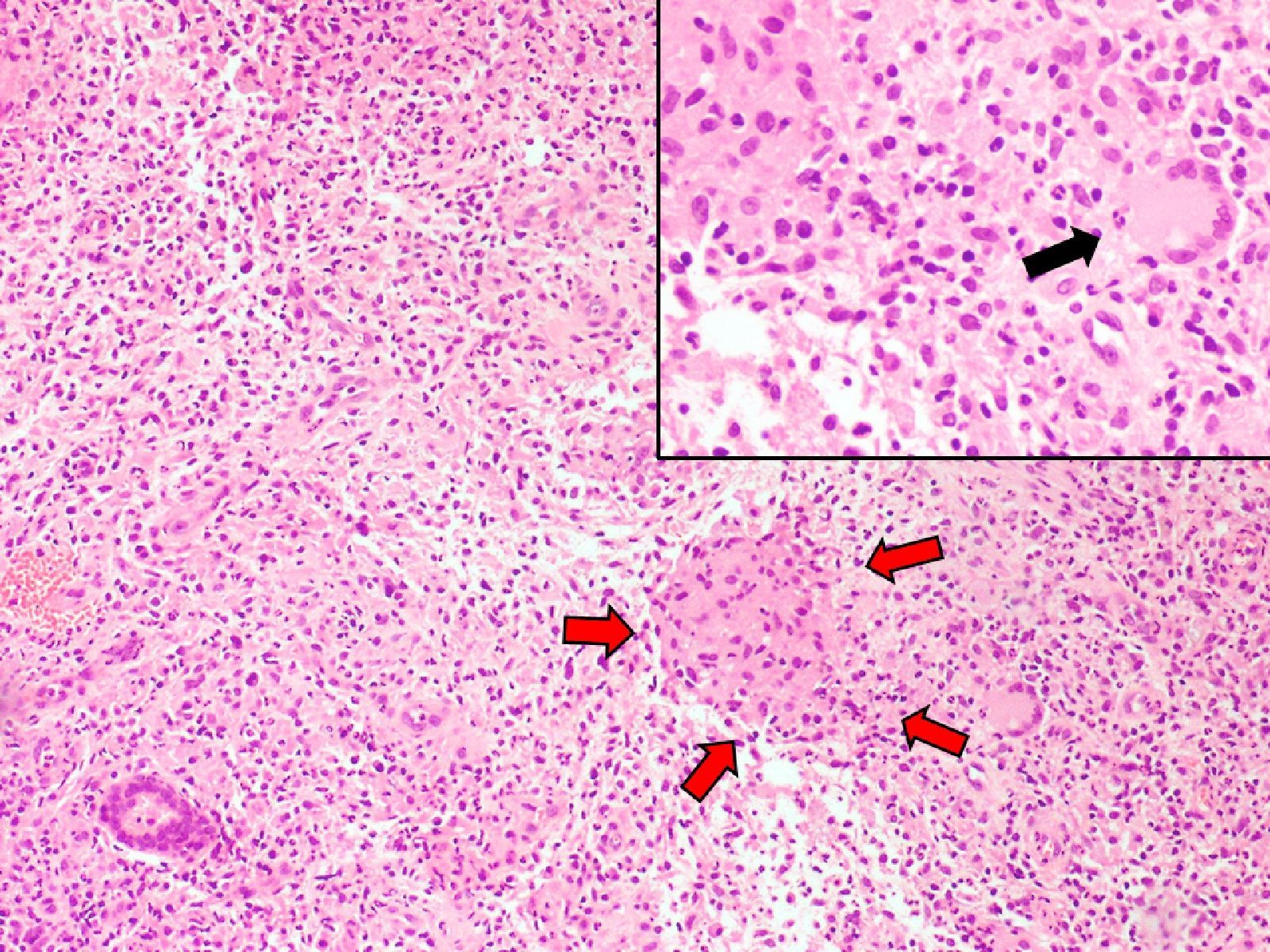
Cultures for bacteria, fungi, and mycobacteria were negative. Histopathologic study of a 3-mm punch biopsy of the lesion revealed marked inflammation affecting the full thickness of the dermis. The inflammatory infiltrate was composed of histiocytes, either isolated or forming poorly defined granulomas, and some multinucleated giant cells interspersed with lymphocytes, plasma cells, and neutrophils. No suppurative granulomas were observed. In addition to hematoxylin-eosin staining, other special techniques involving staining with methenamine silver, periodic acid Schiff, Gram, Ziehl-Neelsen and Fite Faraco were used to rule out an infectious etiology (Fig. 2).
. To the right of this is a multinucleated giant cell (black arrow). Note the higher magnification in top right-hand corner of the image. Hematoxylin-eosin ×20.")
Based on the results obtained, the lesion was diagnosed as an idiopathic facial aseptic granuloma. No treatment was prescribed.
Four months after the first visit, the lesion had completely disappeared, leaving a slightly pink macule in its place (Fig. 3.)

The exact etiology of IFAG is unknown, although Boralevi et al.2 have postulated that these lesions may be related to a granulomatous process around an embryological remnant or may belong to the spectrum of granulomatous rosacea in infants. A prospective multicenter study of 30 cases by the same authors reported the mean duration of the lesions to be 11 months and found antibiotic treatment ineffective.
The principal differential diagnosis for this type of lesion includes benign tumors (especially pilomatricomas of the eyelids or eyebrows,4,5 dermoid or epidermoid cysts, and chalazia), pyogenic granulomas, Spitz nevi, and xanthogranulomas. It is also important to rule out the possibility of a bacterial or fungal infection, or infection with mycobacteria or parasites (leishmaniasis), all of which are more common in immunocompromised patients.2 These lesions can sometimes resemble vascular malformations or hemangiomas, although the clinical course is very different.3 Other differential diagnoses include nodulocystic acne presenting few symptoms.2,6
Our aim in presenting this case is to emphasize the importance of considering IFAG in the differential diagnosis of acquired facial nodules in children. It is important to inform parents of the benign course of these lesions. Follow-up until the lesion resolves is recommended.1
The characteristic clinical appearance and location of IFAG and the lack of lymphadenopathy or constitutional symptoms may make a direct clinical diagnosis possible and thereby avoid unnecessary interventions.
Please cite this article as: Hiraldo-Gamero A, et al. Granuloma aséptico facial idiopático. Actas Dermosifiliogr. 2013;104:635–6.



