

Actinic keratosis (AK) is characterized by intraepidermal proliferations of dysplastic keratinocytes, and is more frequent in men and in individuals with low phototypes.1 Despite its high prevalence and the risk of malignancy, awareness of AK is low among the general population and even among a percentage of primary care physicians (PCPs), and it is considered an underdiagnosed and undertreated problem.2 European guidelines propose an active role of PCPs in treating patients with incipient lesions and referring them for ablative or cancerization field treatment.3 In Spain, these patients are monitored by PCPs and referred to dermatology services in cases of diagnostic doubt or to plan the therapeutic approach.4
We evaluated the factors influencing the decision to treat AK in a sample of PCPs from the public health service of Andalusia, Spain. Based on factors reported in the literature to facilitate or hinder AK treatment, a questionnaire was developed and a focus group conducted with dermatologists and PCPs. The initial version of the questionnaire was evaluated by 10 PCPs to assess comprehension, feasibility, and completion time. The final version consisted of 13 questions, rated using a 5-point Likert scale. Information was collected about years of experience, the use of teledermatology and dermoscopy, hours of training in dermatology, and the level of self-reported dermatological knowledge relative to other PCPs. To assess the association between these variables and the decision to treat AK, a bivariate analysis was performed using either the Chi-squared test (for qualitative variables) or the student t test (for numerical variables). An exploratory factor analysis (EFA) was performed, followed by multivariate logistic regression in which the explanatory variables were those obtained in the EFA and the dependent variable was AK treatment.
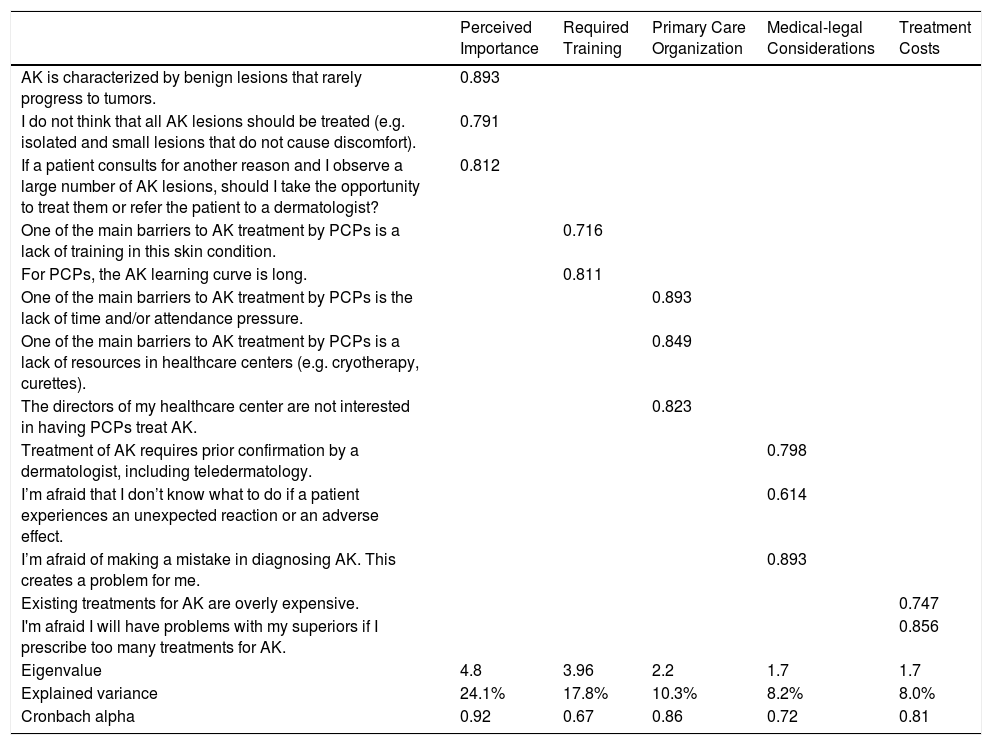
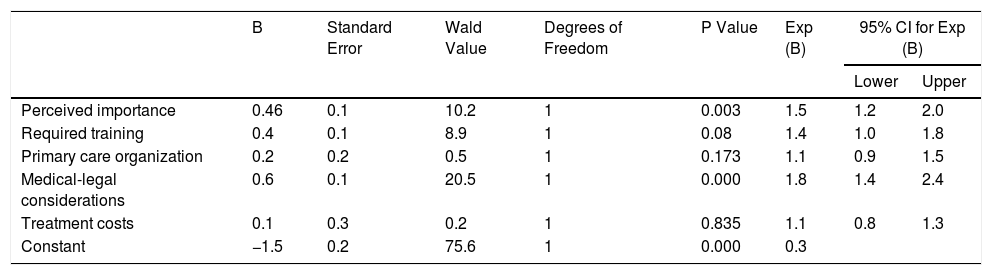
After distributing the questionnaire to 381 PCPs, 98 (25.7%) responded, a response rate similar to that reported for other questionnaires with these characteristics.5 The margin of error was 8.5%, with a 95% confidence interval (95% CI). Only 38.8% (95% CI 29.7–48.7) of PCPs reported that they had treated AK. Teledermatology and dermoscopy were used by 78.6% and 41.2% of respondents, respectively. Most respondents (66.3%) reported a level of dermatological knowledge similar to that of other PCPs. In the preceding 5 years they had received an average of 24.1±44.9 hours of training in dermatology and 7.4±12.1hours dedicated specifically to skin cancer. The only variables that were statistically significant were the use of dermoscopy and self-reported dermatological knowledge. The results of the EFA (Table 1) explained 68.5% of the variance. The Cronbach alpha values (0.67–0.92) obtained confirmed the reliability of the selected determinants of AK treatment: perceived importance, necessary training, primary care organization, medical-legal considerations, and treatment costs. Table 2 shows the results of the logistic regression analysis. Medical-legal considerations was the variable with the greatest explanatory power, followed by perceived importance. Both were found to be direct determinants of the decision to treat AK by PCPs. No association was observed for necessary training, primary care organization, or treatment costs.
Results of the Multivariate Factor Analysis
| Perceived Importance | Required Training | Primary Care Organization | Medical-legal Considerations | Treatment Costs | |
|---|---|---|---|---|---|
| AK is characterized by benign lesions that rarely progress to tumors. | 0.893 | ||||
| I do not think that all AK lesions should be treated (e.g. isolated and small lesions that do not cause discomfort). | 0.791 | ||||
| If a patient consults for another reason and I observe a large number of AK lesions, should I take the opportunity to treat them or refer the patient to a dermatologist? | 0.812 | ||||
| One of the main barriers to AK treatment by PCPs is a lack of training in this skin condition. | 0.716 | ||||
| For PCPs, the AK learning curve is long. | 0.811 | ||||
| One of the main barriers to AK treatment by PCPs is the lack of time and/or attendance pressure. | 0.893 | ||||
| One of the main barriers to AK treatment by PCPs is a lack of resources in healthcare centers (e.g. cryotherapy, curettes). | 0.849 | ||||
| The directors of my healthcare center are not interested in having PCPs treat AK. | 0.823 | ||||
| Treatment of AK requires prior confirmation by a dermatologist, including teledermatology. | 0.798 | ||||
| I’m afraid that I don’t know what to do if a patient experiences an unexpected reaction or an adverse effect. | 0.614 | ||||
| I’m afraid of making a mistake in diagnosing AK. This creates a problem for me. | 0.893 | ||||
| Existing treatments for AK are overly expensive. | 0.747 | ||||
| I'm afraid I will have problems with my superiors if I prescribe too many treatments for AK. | 0.856 | ||||
| Eigenvalue | 4.8 | 3.96 | 2.2 | 1.7 | 1.7 |
| Explained variance | 24.1% | 17.8% | 10.3% | 8.2% | 8.0% |
| Cronbach alpha | 0.92 | 0.67 | 0.86 | 0.72 | 0.81 |
Determinant value, 0.0021.
Kaiser–Meyer–Olkin (KMO) value, 0.724.
Bartlett sphericity test value, 2133.1 (p<0.001).
Abbreviations: AK, actinic keratosis; PCP, primary care physician.
Logistic Regression Analysis: Relationships Between Explanatory Variables and Treatment of AK
| B | Standard Error | Wald Value | Degrees of Freedom | P Value | Exp (B) | 95% CI for Exp (B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Perceived importance | 0.46 | 0.1 | 10.2 | 1 | 0.003 | 1.5 | 1.2 | 2.0 |
| Required training | 0.4 | 0.1 | 8.9 | 1 | 0.08 | 1.4 | 1.0 | 1.8 |
| Primary care organization | 0.2 | 0.2 | 0.5 | 1 | 0.173 | 1.1 | 0.9 | 1.5 |
| Medical-legal considerations | 0.6 | 0.1 | 20.5 | 1 | 0.000 | 1.8 | 1.4 | 2.4 |
| Treatment costs | 0.1 | 0.3 | 0.2 | 1 | 0.835 | 1.1 | 0.8 | 1.3 |
| Constant | −1.5 | 0.2 | 75.6 | 1 | 0.000 | 0.3 | ||
x2, 46.1 (p = 0.000); Hosmer–Lemeshow test, 9.8 (p = 0.077); Nagelkerke R squared, 0.18.
Abbreviations: B, coefficient for the constant in the null model; Exp (B), exponentiation of the B coefficient; 95% CI, 95% confidence interval.
Our analysis allowed us to identify the factors that best explain the decision to treat AK by PCPs. To our knowledge, no such study has been previously carried out in Spain. We found that 38.8% of the respondents opted to treat AK, in line with the proportion (40%) reported by Halpern et al.6 The most relevant determinant of the decision to treat AK was medical-legal considerations (i.e. fear of misdiagnosis or an adverse reaction to treatment). In our opinion, this insecurity could be due to insufficient training and overly heterogeneous guidelines, ultimately leading to a decision not to treat. In fact, the Spanish Society for Healthcare Quality (SECA)7 recently pioneered a circuit of care for AK patients in Spain, and identified the functions of the different agents involved. The authors concluded that a lack of coordinated action is one of the barriers to quality of care in AK, and emphasized the need to protocolize both diagnosis and treatment of AK. We identified perceived importance as the second key factor influencing the decision to treat AK in our sample of PCPs. In general, awareness about AK is low, and is slightly higher in countries with a high AK prevalence such as Australia, where PCPs play a more active role in AK follow-up and treatment.8 Given the chronicity and prevalence of AK, PCPs should be trained to follow up AK patients. This can be facilitated by providing training programs, which have been shown to improve the detection of AK and nonmelanoma skin cancer,9 although in our sample we observed no association between training and the decision to treat AK.
Certain limitations should be borne in mind when interpreting our findings. The use of a nonvalidated ad hoc questionnaire, which was distributed online, the limitation of the study to a single hospital area, and the low response rate (<26%) may limit generalization of the findings.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Pereyra-Rodriguez JJ, Monserrat-García MT, Corbí-Llopis R, Conejo-Mir Sánchez J. Determinantes del tratamiento de las queratosis actínicas por médicos de atención primaria. Actas Dermosifiliogr. 2020;111:444–446.



