





Epidemiologic and disease burden data are essential for disease control and optimal health care resource planning. The aims of this study were to estimate the epidemiologic burden of psoriasis and evaluate associated comorbidities, health care utilization, and sick leave.
Material and methodsWe collected data from the 2016 Catalan Health Survey (ESCA), the Catalan Registry of Morbidity and Utilization of Health Care Services (MUSSCAT) (2016), and the database of the Catalan Medical Evaluations Institute (ICAM) (2012–2016).
ResultsThe prevalence of psoriasis in Catalonia according to 2016 ESCA data is approximately 1.8%.
The MUSSCAT registry data indicate that the incidence has remained stable in recent years. The most common comorbidities associated with psoriasis are hypertension (35%) and diabetes (15%). Forty percent of patients with psoriasis have a moderate to high risk for death or high health resource utilization. Annual use of resources by psoriasis patients is high: they make a mean of 8.7 primary care visits, 2.8 outpatient visits, 0.5 emergency and day hospital visits, 0.2 mental health visits, and use 6.1 medications.
Sick leave due to psoriasis or psoriatic arthritis accounted for 0.04% of all cases.
ConclusionsThe prevalence of psoriasis in Catalonia is high at 1.8%. The disease burden is also high, both in terms of comorbidities and health care utilization.
Disponer de datos epidemiológicos y de carga de una enfermedad es crucial para su control y óptima planificación. El objetivo es estimar la carga de la psoriasis en términos epidemiológicos, comorbilidades asociadas, uso de recursos sanitarios e incapacidad laboral.
Material y métodoSe han analizado los datos de la Encuesta de Salud de Cataluña (ESCA) de 2016, el Registro de Morbilidad y Utilización de Servicios Sanitarios de Cataluña (MUSSCAT) de 2016 y los datos recopilados entre 2012-2016 del Sistema Integrado de Gestión de la Incapacidad Temporal del Instituto Catalán de Evaluaciones Médicas.
ResultadosLa prevalecía de la psoriasis en Cataluña en base a los datos de la ESCA se sitúa en el 1,8%.
Los datos de MUSSCAT muestran que el número de casos incidentes se ha mantenido estable en los últimos años. Las comorbilidades más frecuentes en el paciente con psoriasis son la hipertensión arterial (35%) y la diabetes (15%). La estratificación de la población con psoriasis por estratos de riesgo situó al 40% en riesgo moderado-alto. El uso de recursos sanitarios anual de la población con psoriasis es elevado (8,7 visitas atención primaria; 2,8 consultas externas; 0,5 urgencias y hospital de día; 0,2 salud mental; y 6,1 medicamentos).
Los procesos de incapacidad temporal asociados a la psoriasis o artropatía psoriásica representaron el 0,04% del total de registros.
ConclusionesLa prevalencia de la psoriasis en Cataluña es del 1,8%. La carga de la enfermedad es elevada, tanto en términos de comorbilidades del paciente como en el requerimiento de uso de recursos.
Psoriasis is a chronic immune-mediated inflammatory skin disease associated with deregulation of the innate and adaptive immune response in which both genetic and environmental factors are involved.1 It is associated with a number of comorbid conditions, including psoriatic arthritis, metabolic syndrome, cardiovascular disorders, and an increased risk for anxiety, depression, and suicidal ideation. It is also linked to an increased probability of developing inflammatory bowel disease (up to four times that of the general population) and an increased susceptibility to certain malignant tumors.2,3 The management of psoriasis is complicated by the presence of these comorbidities, which contribute to the substantially higher morbidity and mortality found in this group of patients.4
Psoriasis has a considerable physical, emotional, and social impact on those affected,4 leading to a deterioration in their health-related quality of life.5 It also represents a high economic burden for society. While the direct cost of care accounts for the largest proportion of the total burden, the costs associated with unemployment and loss of productivity are also substantial: the mean loss of work-related productivity for a patient with psoriasis is estimated to be between 10.1% in the case of mild disease, rising to 29.4% in the most severe cases.6
Having quality epidemiologic data and information on the burden and impact of a disease on our health system affords us a better understanding of the magnitude and distribution of the problem and is key to ensuring its control and adequate health resource planning.
A systematic review of global epidemiologic data on psoriasis undertaken for the World Health Organization (WHO) reported estimates of prevalence ranging from 0.51% to 11.43%. This finding highlights the great variability that exists between different territories,7 making it difficult to draw general conclusions. The differences have been attributed to geographical and environmental factors and to ethnic diversity between different regions; the situation is further complicated by the absence of standardized diagnostic criteria and differences in the methodologies used by different authors.7 In Spain, 2 epidemiologic studies based on telephone surveys conducted in 2001 and 2014 estimated the prevalence of psoriasis at 1.43%8 and 2.3%,9 respectively; this considerable difference is not explained by any unexpected increase in incidence. A recent epidemiologic study based on data from a digital database of medical records relating to the population of a single Spanish region (Lleida) revealed a prevalence of 1.72%; in that study 7.27% of patients with psoriasis were classified as having moderate to severe disease (defined as a need for systemic treatment).10
The objective of the present study was to estimate the burden of psoriasis in Catalonia in terms of epidemiology, comorbid conditions, health resource use, and work-related disability on the basis of data recorded in the databases of the Catalan Department of Health.
Material and MethodsWe analyzed data from three Catalan databases: the 2016 Catalan Health Survey (ESCA), the Catalan Registry of Morbidity and Utilization of Health Care Services (MUSSCAT) (2016), and the database of the Catalan Medical Evaluations Institute (ICAM) (data collected between 2012 and 2016).
Catalan Health SurveyESCA is a tool that has been used by the Catalan Department of Health since 1994 to obtain data on the Catalan population required to inform the development and evaluation of policies to be included in the Catalan Health Plan.11 The survey, which is not age limited, is designed to collect information on the health status, health-related behaviors, and health service utilization of the non-institutionalized population living in Catalonia.12
The cross-sectional survey collects information from a representative sample of the population of Catalonia through home interviews, often carried out twice yearly.12 The sample is selected using random, multistage, stratified sampling methods and is designed to be representative in terms of sex, age, and the size of the non-institutionalized population of the municipality.
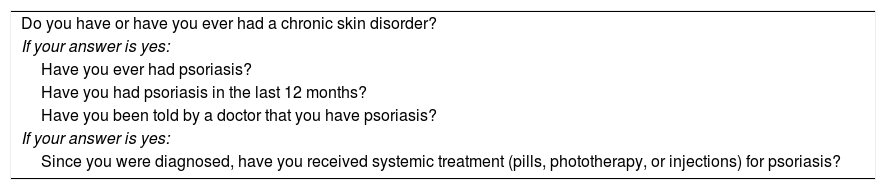
Estimated Prevalence of PsoriasisWe estimated the prevalence of psoriasis in Catalonia on the basis of the responses of the population aged 15 years or older to the questions in the 2016 ESCA survey (Table 1).
Questions Included in the ESCA Survey to Ascertain the Prevalence of Psoriasis in Catalonia.
| Do you have or have you ever had a chronic skin disorder? |
| If your answer is yes: |
| Have you ever had psoriasis? |
| Have you had psoriasis in the last 12 months? |
| Have you been told by a doctor that you have psoriasis? |
| If your answer is yes: |
| Since you were diagnosed, have you received systemic treatment (pills, phototherapy, or injections) for psoriasis? |
The prevalence of the disease and the corresponding confidence intervals have been calculated for the total population and by sex.
We used either Fisher’s exact test or Pearson’s X2 test, as appropriate, to establish the association between chronic skin problems and sex. A significance level of 95% was used in all the analyses, taking into account the complexity of the sample design. The statistical analysis was performed using IBM’s SPSS Statistics version 24.0.0 and Microsoft Excel.
Catalan Registry of Morbidity and Utilization of Health Care ServicesWe analyzed data relating to 2016 taken from the MUSSCAT database maintained by the Catalan Health Service (CatSalut), a registry that includes detailed information on the use by the population of Catalonia of publicly-funded health care services. MUSSCAT combines information from several public databases using each individual’s unique identifier as the connecting link. It includes all the basic minimum data sets as well as information on drug prescription issues and billing records.13
Estimated Incidence and Prevalence of PsoriasisWhile this database was not designed to facilitate the calculation of disease prevalence or incidence, the data can be used to make estimates given that each individual is identified by a unique key. The data does, therefore, allow us to calculate prevalence and incidence, at least among the set of people who have used a health resource and whose case has been assigned an international disease classification (ICD) code specifying a particular disease. Using this data, it was possible to estimate the prevalence of psoriasis in 2016 in the population alive at the end of the year classified with a diagnosis of psoriasis (ICD-9-CM codes 696.0, 696.1 and 696.8) and reported by a health service at any level (primary care, hospitals, mental health, and residential healthcare (elder care, nursing home, etc.). Individuals whose diagnosis was first reported during 2016 were considered to represent new cases (incidence).
Description of the Population Diagnosed with PsoriasisThe descriptive analysis of the population with psoriasis recorded in the MUSSCAT database in 2016 included the percentages of men and women, median age and interquartile range, the frequency of comorbid conditions, and stratified distribution by risk of mortality and/or a high level of health resource use.
The method used to stratify the population by risk was first to define adjusted morbidity groups classifying the population into 6 groups and then to classify these groups into 5 levels of complexity, along with 1 healthy population group.14,15
The X2 test was used to analyze comorbidities and sex. However, the Kruskall-Wallis test was used to analyze age because of the non-normal distribution of the data for this variable, which was determined using the Shapiro-Wilks test.
Estimate of Resource Use and Associated Costs for Patients Diagnosed With PsoriasisThe data on the cases involving a diagnosis of psoriasis during 2016 registered on MUSSCAT were analyzed to calculate the use of health care resources by patients with psoriasis. The following resources were analyzed: 1) the use of outpatient medical resources (emergency room visits, mental health services, day hospital, outpatient consultations, and primary care visits) and number of prescribed medications; and 2) placement in a residential, psychiatric or hospital facility.
The results are presented as cost per patient for the use of outpatient resources and cost per 100 patients in the case of inpatient services.
All the analyses of MUSSCAT data were carried out using statistical package R version 3.4.2.
ICAM Integrated Disability Management System DatabaseAll episodes of temporary incapacity for work due to illness are registered on an ICAM database. The primary diagnosis motivating such sick leave is coded using the World Health Organization ICE-9 or ICE-10 system (depending on the primary health care provider reporting the episode).
Estimated Burden of Sick Leave Due to PsoriasisTo determine the impact of psoriasis on the frequency of sick leave in the Catalan population between 2012 and 2016, we counted all episodes recorded during that period for which the primary complaint was a diagnosis of psoriasis or psoriatic arthritis (CIE-9 codes 696.0 and 696.1 and CIE-10 codes L40.0, L40.1, L40.4, L40.5, L40.8, and L40.9). We also determined the number of days leave for each episode.
ResultsPrevalence of PsoriasisIn 2016, the ESCA survey included data from 4818 people, of whom 3877 (1910 men and 1967 women) were aged 15 years or older.
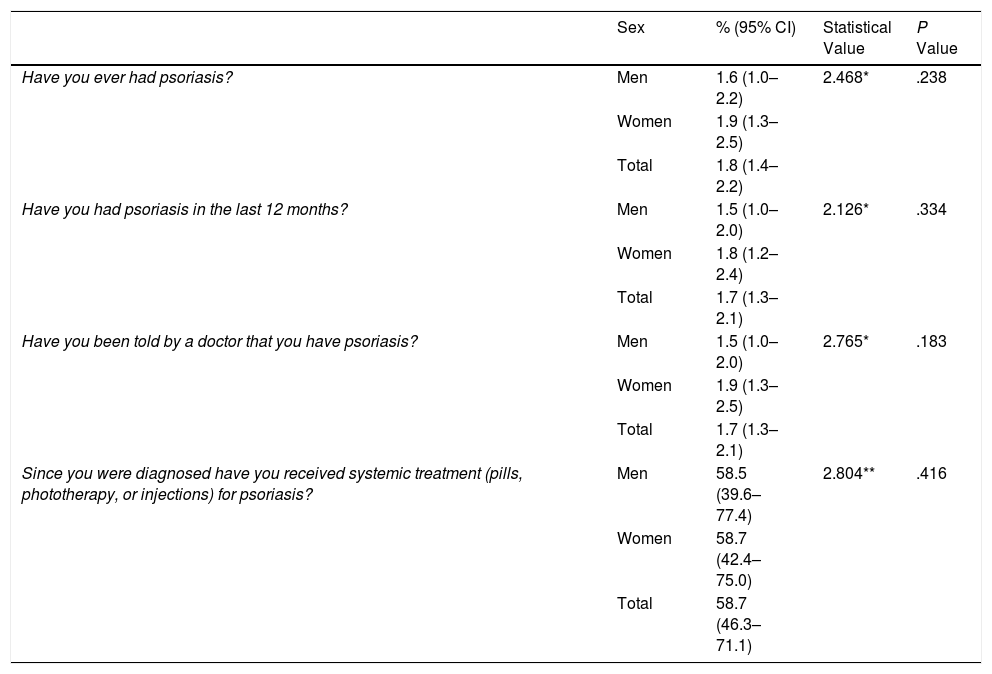
According to the ESCA data, 1.8% (95% CI, 1.4-2.2) of the non-institutionalized population living in Catalonia aged 15 years or older reported having had psoriasis at some time, and 1.7% (95% CI, 1.3-2.1) reported an episode in the preceding 12 months. Moreover, 1.7% of respondents reported that a doctor had informed them that they had psoriasis. Of these, 58.7% reported receiving systemic treatment for the disease. No significant sex-related differences were observed (Table 2).
ESCA Results in the Population Aged 15 Years or Older.
| Sex | % (95% CI) | Statistical Value | P Value | |
|---|---|---|---|---|
| Have you ever had psoriasis? | Men | 1.6 (1.0–2.2) | 2.468* | .238 |
| Women | 1.9 (1.3–2.5) | |||
| Total | 1.8 (1.4–2.2) | |||
| Have you had psoriasis in the last 12 months? | Men | 1.5 (1.0–2.0) | 2.126* | .334 |
| Women | 1.8 (1.2–2.4) | |||
| Total | 1.7 (1.3–2.1) | |||
| Have you been told by a doctor that you have psoriasis? | Men | 1.5 (1.0–2.0) | 2.765* | .183 |
| Women | 1.9 (1.3–2.5) | |||
| Total | 1.7 (1.3–2.1) | |||
| Since you were diagnosed have you received systemic treatment (pills, phototherapy, or injections) for psoriasis? | Men | 58.5 (39.6–77.4) | 2.804** | .416 |
| Women | 58.7 (42.4–75.0) | |||
| Total | 58.7 (46.3–71.1) |
The MUSSCAT data show that the cumulative incidence of psoriasis has remained virtually stable in recent years, with about 1.4 cases per 1000 inhabitants per year; 22 043 new cases were reported in 2016 (Fig. 1).
Profile of the Patient with Psoriasis in MUSSCAT
In the MUSSCAT data, we found a prevalence of 136 466 cases of psoriasis, that is 1.83 cases per 100 inhabitants. Of these, 53.6% were men. This estimate calculated using health resource utilization data is consistent with the estimate calculated on the basis of the ESCA survey results.
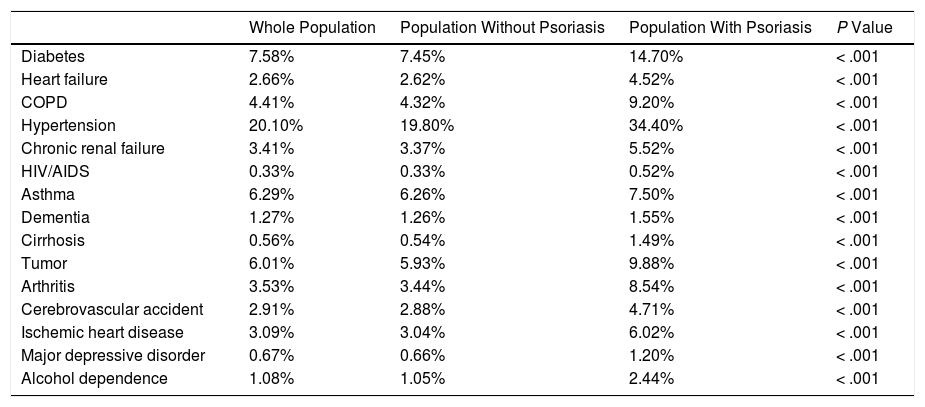
The most common comorbid diseases found in the patients with psoriasis were hypertension (35%) and diabetes (15%). The proportions of patients with tumors, chronic obstructive pulmonary disease (COPD), or arthritis were all around 9% (Table 3). The prevalence of all the comorbid diseases studied was higher in the group of patients with psoriasis than in the population as a whole.
Main Comorbid Diseases in Patients with Psoriasis.
| Whole Population | Population Without Psoriasis | Population With Psoriasis | P Value | |
|---|---|---|---|---|
| Diabetes | 7.58% | 7.45% | 14.70% | < .001 |
| Heart failure | 2.66% | 2.62% | 4.52% | < .001 |
| COPD | 4.41% | 4.32% | 9.20% | < .001 |
| Hypertension | 20.10% | 19.80% | 34.40% | < .001 |
| Chronic renal failure | 3.41% | 3.37% | 5.52% | < .001 |
| HIV/AIDS | 0.33% | 0.33% | 0.52% | < .001 |
| Asthma | 6.29% | 6.26% | 7.50% | < .001 |
| Dementia | 1.27% | 1.26% | 1.55% | < .001 |
| Cirrhosis | 0.56% | 0.54% | 1.49% | < .001 |
| Tumor | 6.01% | 5.93% | 9.88% | < .001 |
| Arthritis | 3.53% | 3.44% | 8.54% | < .001 |
| Cerebrovascular accident | 2.91% | 2.88% | 4.71% | < .001 |
| Ischemic heart disease | 3.09% | 3.04% | 6.02% | < .001 |
| Major depressive disorder | 0.67% | 0.66% | 1.20% | < .001 |
| Alcohol dependence | 1.08% | 1.05% | 2.44% | < .001 |
COPD: chronic obstructive pulmonary disease; HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome.
In line with this higher frequency of comorbid disease, stratification of the population with psoriasis by risk of mortality and/or substantial health resource use showed that 40% were at moderate to high risk (Fig. 2).
Resource Use and Associated Cost
Utilization of health care resources was higher among patients with psoriasis than in the general population. In 2016, individuals with psoriasis in the MUSSCAT data set made an average of 8.7 visits to their primary care physician, 2.8 outpatient consultations, 0.5 visits to an emergency room or day hospital, and 0.2 visits to a mental health service. They also required more different prescription medicines than members of the general population (Fig. 3).

The rate of admission to residential, psychiatric, and acute care facilities were 1.9, 0.4 and 18.0 per 100 patients, respectively. These rates are slightly higher than those found in the population as a whole (Fig. 4).
Sick Leave
In the period from 2012 to 2016, episodes associated with psoriasis or psoriatic arthritis accounted for 0.04% of all sick leave episodes and 0.11% of all days of leave due to temporary incapacity among non-professionals in Catalonia.
DiscussionThe prevalence of psoriasis in the population of Catalonia in 2016 was 1.8%, a very different figure than earlier estimates made in 2001 (1.2%)8 and 2014 (2.5%).9 The prevalence estimated from the results of the ESCA survey and that obtained from the MUSSCAT data coincide and both appear to be more consistent with the latest estimates published in 2018 (1.72%).10 The estimated prevalences reported in other countries in the region are higher: 2.7% in Italy16 and 5.17% in France.17 These differences may be due to the different methodologies used in each country and to the definition of prevalence and the diagnostic criteria for psoriasis used in the different studies. In Italy, in-person interviews were conducted with a randomly chosen sample population during which the participants were asked about their history of skin diseases, including psoriasis, and data was collected on treatment, age at diagnosis, and duration of disease. The respondents also specified whether they had received a diagnosis of psoriasis from a doctor. In France, the estimated prevalence was based on responses to a questionnaire sent to a representative sample of the French population comprising 10 000 individuals. The respondents indicated whether they had had an episode of psoriasis in the preceding 12 months, but no doctor’s diagnosis was required.
The profile of the patient with psoriasis identified in this study is in line with the results of earlier studies carried out in Spain.10 The results of the present study revealed a numerically higher prevalence among women, but the difference was not statistically significant. There is some debate in the literature regarding the relationship between male sex and an increased risk of developing psoriasis. While the association has been observed by a number of authors,9,10 in other studies, including the present analysis, no significant difference between the sexes in estimated prevalence has been observed.8
There is ample evidence in the literature on the higher prevalence of comorbid diseases in patients with psoriasis.2,3 The MUSSCAT data show the prevalence of all the comorbid diseases to be higher in the population of people with psoriasis than in the general population or among people who do not have psoriasis. However, when interpreting the data on statistical significance, it is important to bear in mind that the MUSSCAT data set is population-based, which means that small differences can be significant.
High blood pressure and diabetes were the 2 most common comorbid conditions in patients with psoriasis. This finding is in line with the results of other studies, which show a relationship between moderate to severe psoriasis and cardiovascular risk factors, such as diabetes and hypertension.18–20 Tumors are the third most common comorbidity in patients with psoriasis. The increased cancer risk the population with psoriasis compared to the general population has been evaluated in a systematic review of the literature and a meta-analysis of 37 studies,21 which showed that patients with psoriasis had a higher risk of developing solid tumors, non-Hodgkin lymphoma, cutaneous squamous cell carcinoma, and basal cell carcinoma. Psoriatic arthritis is one of the main comorbid diseases; it is estimated that about 15% of patients with psoriasis have undiagnosed psoriatic arthritis.22 In our sample, approximately 8% of patients with psoriasis also had arthritis. Respiratory tract diseases have also been associated with psoriasis23; in our study, COPD was the fourth and asthma the sixth most common comorbid disease. Finally, ischemic heart disease and chronic heart failure were among the ten most common comorbidities, a finding in line with studies that have demonstrated a link between psoriasis and increased risk for cardiovascular disease.2,3
Stratification of the population with psoriasis in Catalonia by risk of mortality and/or high utilization of health resources showed that a greater proportion of these patients are at high or moderate risk as compared to the general population. This risk analysis provides information about future needs in terms of health care resources, allowing us to plan for such needs and to develop proactive strategies to meet the demand.
The presence of these comorbid diseases represents a challenge for the management of psoriasis. First, they can limit possible therapeutic options, which may be contraindicated in certain patients. Second, they can give rise to a need for concomitant medication, making it vital to avoid drug interactions in the choice of treatments for psoriasis. Finally, the presence of certain comorbidities may directly influence the therapeutic decisions made by the physician.24 Given its complexity, the management of patients with psoriasis requires a holistic approach and the involvement of various specialties. The pattern of resource use in this setting, as described in this study, demonstrates the need for a multidisciplinary approach. Thus, compared to the general population, patients with psoriasis require more visits to a primary care physician, specialist (outpatient consultations and day hospital visits), and mental health services. Of particular note is the heavy use of the primary care system, with on average more than 8 visits per year; this is an aspect that warrants further study to ascertain why this happens.
The present study shows that psoriasis has a negative impact on the work-related productivity of these patients: psoriasis was cited as the main cause in 0.04% of the cases of sick leave recorded in Catalonia between 2012 and 2016. Moreover, it is possible that the data available may actually underestimate the impact of the disease on productivity, since in many patients the sick leave is linked to arthritis. In the case of leave motivated by psoriatic arthritis, the physician may assign non-specific arthritis codes to the case, which would mean that it would not be classified as psoriasis in the analysis. While there is only limited data on loss of productivity associated with psoriasis, some international studies have shown that these patients are more likely to miss work for health-related reasons (P < 0.05) and have a greater degree of impairment in work productivity (P < 0.001) and impairment in non-work activities (P < 0.001) than people who do not have this disease.25 Similarly, other studies indicate that 49% of patients with active disease are absent from work on a regular basis due to sick leave motivated by psoriasis.26 Disease severity has a negative impact on both direct costs and work-related productivity. This was shown in a recent study that indicated an average loss of work productivity of 10.1% in patients with mild psoriasis, rising to 29.4% in patients with moderate to severe disease.6
LimitationsThe principal limitations of this study are those inherent in the method used to estimate prevalence on the basis of health survey results. The use of self-reported patient data can lead to a concealment bias, common in skin diseases, and also to a possible classification bias (patients were asked whether or not a physician had told them that they have psoriasis). It can also lead to an information bias, such as the one that would explain the difference between the percentage of patients receiving systemic medication in the study by Fernández-Armenteros et al10 (7.2%) compared to the percentage in the ESCA data (58.7%). While the data in the former study was based on the prescriptions recorded in the patients’ medical history, the ESCA data are patient-reported and cannot be subsequently checked with hospital records, a method that may give rise to an information bias.
Despite these limitations, it is important to note that the representativeness of the sample for the population living in Catalonia and the consistency of the results obtained with those of previous studies using other methodologies lends robustness to the findings.
Another possible limitation might be the quality of the information obtained from the databases of public institutions. This quality is guaranteed by automated validation systems that verify the consistency of the data and identify any errors. With respect to the impact of psoriasis on patients’ work-related productivity, it is important to bear in mind that having a disease or condition does not in itself constitute sufficient cause for official sick leave unless the individual’s ability to carry out their work is significantly impaired. Furthermore, only the condition deemed to represent the principal cause of the impairment is cited on the sick leave report. It is, therefore, impossible to rule out the possibility that in the case of many patients with psoriasis who experience psychological effects (stress, depression, anxiety), these may be cited as the reason for the sick leave or temporary disability, obscuring the fact that psoriasis is the underlying cause of their condition. Even with these limitations, the fact that the data used is population-based, individualized, and based on a unique identifier strengthens the results and demonstrates the impact of psoriasis in real-life clinical practice, with the same level of robustness as with the other diseases included in the ESCA and in the health plans.
Finally, it is important to note that the results of this study correspond to a specific Autonomous Community in Spain and a particular time period. This means that extrapolations to the population of Spain as a whole must be approached with caution.
ConclusionsThe prevalence of psoriasis in Catalonia is 1.8%. The burden of the disease is high, in terms of both comorbidity and health resource utilization. The disease also has an appreciable impact on work-related productivity and absenteeism, although the true extent of this may be partly obscured by comorbid conditions, particularly those linked to the emotional impact of psoriasis.
Conflicts of InterestL. Puig has served as a consultant or paid speaker for and/or has participated in clinical trials sponsored by Abbvie, Almirall, Amgen, Baxalta, Biogen, Boehringer Ingelheim, Celgene, Gebro, Janssen, JS BIOCAD, Leo-Pharma, Lilly, Merck-Serono, MSD, Mylan, Novartis, Pfizer, Regeneron, Roche, Sandoz, Samsung-Bioepis, Sanofi, and UCB.
C. Ferrandiz has served as a consultant or paid speaker for and/or has participated in clinical trials sponsored by Abbvie, Almirall, Biosphereium, Celgene, Janssen, Leo-Pharma, Lilly, Merk-Serono, Novartis, Pfizer, Regeneron, Sandoz, Sanofi, and UCB.
R.M. Pujol has participated in clinical trials sponsored by Abbvie, Almirall, Amgen, Biogen, Boehringer Ingelheim, Celgene, Janssen, JS, Leo-Pharma, Lilly, Merck-Serono, MSD, Novartis, Pfizer, Premier Research, Regeneron, Roche, Sandoz, Sanofi, and UCB.
C. Blanch is a full-time employee of Novartis Pharmaceutica S.A.
E. Vela, C. Albertí-Casas, and M. Comellas declare that they have no conflicts of interest.
Please cite this article as: Puig L, Ferrándiz C, Pujol RM, Vela E, Albertí-Casas C, Comellas M, et al. Carga de la psoriasis en Cataluña: datos epidemiológicos, comorbilidades asociadas, uso de recursos sanitarios e incapacidad laboral. Actas Dermosifiliogr. 2021;112:425–433.



