

Anogenital wart (AGW) resulting from human papilloma virus (HPV) is one of the most common sexually transmitted diseases worldwide. Herein, we aimed to evaluate the effects of AGW on patients‘marital satisfaction and sexual function. This cross-sectional study was consisted of 74 consecutive patients including 37 patients with AGW and 37 healthy controls. ENRICH Marital Satisfaction Scale and Arizona Sexual Experience Scale were completed and analyzed for all patients. ENRICH scale items were not significantly different between the two groups. Sexual function was found to be lower in female than male patients (P<.001). According to our findings marital satisfaction was not affected by AGW. However, a history of previous treatment for HPV decreased the marital satisfaction. In addition, AGW had more adverse effects on females’ sexual function compared to males. Our findings suggest that the psychiatric treatments should be considered when managing an AGW patient.
Las verrugas anogenitales (VAG) debidas al virus papiloma humano son una de las enfermedades de trasmisión sexual más comunes en todo el mundo. El objetivo de este trabajo fue evaluar los efectos de las VAG en la satisfacción matrimonial y en la actividad sexual de los pacientes. Presentamos un estudio transversal que incluyó 74 pacientes consecutivos, de los cuales 37 presentaban VAG y los 37 sujetos restantes eran controles sanos. Todos los pacientes completaron y fueron analizados por la Escala de satisfacción matrimonial de ENRICH y la Escala Arizona de experiencias sexuales. Los ítems de la escala ENRICH no mostraron diferencias significativas entre los 2 grupos. La actividad sexual fue menor en las mujeres que en los hombres (p<0,001). De acuerdo con nuestros hallazgos la satisfacción conyugal no se vio afectada por las VAG. Sin embargo, el tratamiento previo del virus del papiloma humano redujo la satisfacción marital. A todo ello hay que añadir que la VAG mostró más efectos adversos sobre la actividad sexual de las mujeres que sobre la de los hombres. Nuestros hallazgos sugieren que se debe considerar el uso de tratamientos psiquiátricos en el manejo del paciente con VAG.
Sexual transmitted diseases (STDs) are mostly caused by human papilloma virus (HPV). HPV is frequently observed in general population, in fact it affects 75% of sexually active women. Most of HPV victims are aged between 18 to 25. HPV is often asymptomatic and usually self-limited (70-90%).1
During recent past years, various aspects of anogenital warts (AGWs) have been discussed. However, few studies have concerned the effects of genital wart diagnosis on psychosocial and psychosexual parameters.
Previous investigations on women with abnormal PAP test reflected their psychosocial issues such as: anxiety, fear of cancer, sexual and reproductive complications2,3 sense of anger, social stigma and hypochondria.4 Clarke et al.5 reported embarrassment, frustration, isolation, fear of depilation as primary responses to HPV diagnosis. Besides the adverse psychological effects, fear of genital examination, worry about transmitting the disease to the partner and fear of stigmatization by the sexual partner were very prevalent. When informed about HPV infection, many patients felt less sexually attractive and were not satisfied with their sexual intercourse. However, these results are challenged by other studies. Reed et al. claimed that sexual function and psychosexual variables were not different between women with AGW and healthy controls.6
Evidence about the impact of AGW on marital satisfaction and sexual function are scarce and controversial. On the other hand, few studies have addressed this issue in Iran, despites its high prevalence in the country.7 Furthermore, Iranian population have distinct cultural, social and religious differences from western societies, which directly influence the self-image of AGW patients. So, this study was aimed to investigate the marital satisfaction and sexual function in AGW patients in an Iranian sample.
Clinical cases and methodsWe recruited 74 individuals into this cross sectional study including 37 patients with AGW and 37 healthy controls. The presence of AGW was confirmed by dermatologist on the basis of clinical presentations. The study was conducted in Imam Reza hospital at Mashhad University of Medical Sciences (MUMS) in 2014. Patients were aged from 18 to 64 years. Both groups were matched according to age, gender, education and marital status. All participants were informed about the study process by written consent approved by the ethical committee of MUMS. We excluded cases with the history of psychopathological conditions and the existence of any underlying medical condition. Demographic data, marital status, education, occupation, duration of the disease, history of prior treatment for AGW, localization of the warts, presence of medical comorbidities, and history of psychiatric visit were recorded.
ENRICH Marital Satisfaction Scale 35 itemsThis scale is short form of a 115-question list which was prepared by Fowres and Olson (2006). This questionnaire is a self-administered tool for measuring the alterations of marriages as well as the ratio of marital satisfaction, marital relationship, conflicts solving and ideal distortions. The validity and reliability of the ENRICH questionnaire were confirmed by Fowers et al. (Alpha coefficient=0).8
Arizona Sexual Experience Scale (ASEX)This questionnaire includes five items including: sexual drive, sexual arousal, lubrication/erection, orgasm and sexual satisfaction, with options graded as: extremely easy, very easy, somewhat easy, somewhat difficult, very difficult and never. The maximum score is 30 and the minimum score is 5. Higher scores indicate higher sexual dysfunction. The reliability and validity of ASEX questionnaire is confirmed by Mc Gahuey et al.9
Statistical analysisIndependent-samples t-test, Mann Whitney U test, and Chi Square test were used to find the significant differences; p-values less than 0.05 were considered statistically significant. All analyses were conducted using SPSS version 16.0.1 for Windows.
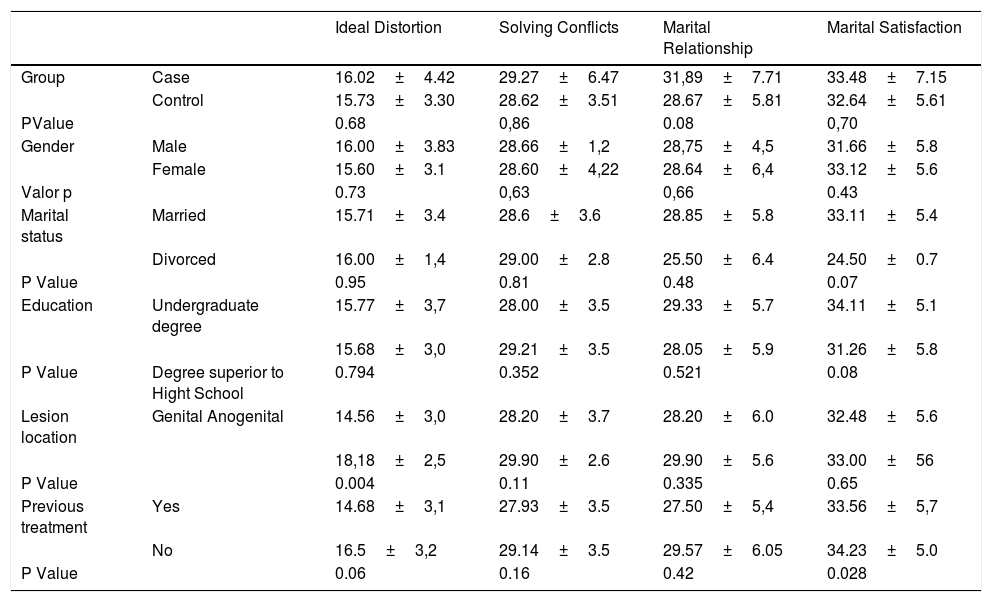
ResultsThe baseline characteristics of participants are shown in Table 1. ENRICH scale items were not significantly different between the two groups (Table 2). Marital status, level of education and lesion location did not considerably affect the ENRICH scale items in the case group. However, our data showed that patients with the history of previous treatment of AGW had lower marital satisfaction (p=0.028). Detailed data of the ENRICH scale findings are presented in Table 2.
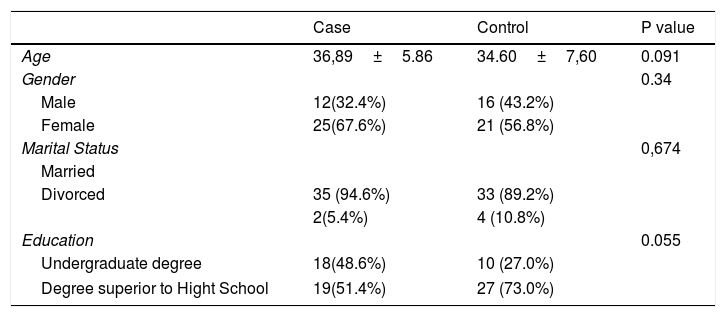
Demographic data of patients with anogenital wart (AGW) compared to healthy controls.
| Case | Control | P value | |
|---|---|---|---|
| Age | 36,89±5.86 | 34.60±7,60 | 0.091 |
| Gender | 0.34 | ||
| Male | 12(32.4%) | 16 (43.2%) | |
| Female | 25(67.6%) | 21 (56.8%) | |
| Marital Status | 0,674 | ||
| Married | |||
| Divorced | 35 (94.6%) | 33 (89.2%) | |
| 2(5.4%) | 4 (10.8%) | ||
| Education | 0.055 | ||
| Undergraduate degree | 18(48.6%) | 10 (27.0%) | |
| Degree superior to Hight School | 19(51.4%) | 27 (73.0%) | |
The comparison of ENRICH scale items between the study groups.
| Ideal Distortion | Solving Conflicts | Marital Relationship | Marital Satisfaction | ||
|---|---|---|---|---|---|
| Group | Case | 16.02±4.42 | 29.27±6.47 | 31,89±7.71 | 33.48±7.15 |
| Control | 15.73±3.30 | 28.62±3.51 | 28.67±5.81 | 32.64±5.61 | |
| PValue | 0.68 | 0,86 | 0.08 | 0,70 | |
| Gender | Male | 16.00±3.83 | 28.66±1,2 | 28,75±4,5 | 31.66±5.8 |
| Female | 15.60±3.1 | 28.60±4,22 | 28.64±6,4 | 33.12±5.6 | |
| Valor p | 0.73 | 0,63 | 0,66 | 0.43 | |
| Marital status | Married | 15.71±3.4 | 28.6±3.6 | 28.85±5.8 | 33.11±5.4 |
| Divorced | 16.00±1,4 | 29.00±2.8 | 25.50±6.4 | 24.50±0.7 | |
| P Value | 0.95 | 0.81 | 0.48 | 0.07 | |
| Education | Undergraduate degree | 15.77±3,7 | 28.00±3.5 | 29.33±5.7 | 34.11±5.1 |
| 15.68±3,0 | 29.21±3.5 | 28.05±5.9 | 31.26±5.8 | ||
| P Value | Degree superior to Hight School | 0.794 | 0.352 | 0.521 | 0.08 |
| Lesion location | Genital Anogenital | 14.56±3,0 | 28.20±3.7 | 28.20±6.0 | 32.48±5.6 |
| 18,18±2,5 | 29.90±2.6 | 29.90±5.6 | 33.00±56 | ||
| P Value | 0.004 | 0.11 | 0.335 | 0.65 | |
| Previous treatment | Yes | 14.68±3,1 | 27.93±3.5 | 27.50±5,4 | 33.56±5,7 |
| No | 16.5±3,2 | 29.14±3.5 | 29.57±6.05 | 34.23±5.0 | |
| P Value | 0.06 | 0.16 | 0.42 | 0.028 |
Duration of the disease was also significantly correlated with several ENRICH items including: marital relationship (r=0.57, p<0.01), solving conflicts (r=0.33, p<0.05) and ideal distortion (r=0.35, p<0.05). Conversely, our data failed to show any correlation between marital satisfaction, age and multiple marriages in the case group.
Sexual function was found to be lower in females than males in patients (p<0.001). The level of education was not significantly different between AGW patients. Sexual dysfunction was more deteriorated in unemployed people and housewives compared to self-employed patients and government employees (p<0.05).
DiscussionHPV is a common finding in most sexually transmitted infections (STIs) and results in psychological ailments and physical inconvenience.10 Though literature is more focused on the psychological and psychosexual aspects of AGW. This study as we know is the first study reporting the impact of AGW on marital satisfaction and sexual function in Iran.
According to our data AGW did not have significant effects on marital satisfaction. However, the duration of the disease significantly decreased several ENRICH scale items including: marital relationship, solving conflicts and ideal distortion.
The history of previous treatment decreased the marital satisfaction. This is perhaps because of prolix process of HPV treatment and concerns about the disease recurrence. Furthermore, multiple interventions are showed to diminish the psychosocial aspects of the disease.4,11 Filiberti et al. evaluated the effects of HPV treatment on psychosexual factors of the patients. 57% of the patients suffered from decreased sexual function after treatment. Sexual dysfunction was mainly caused by painful intercourse and fear of infecting the partner. Also 16% of patients complained about deteriorated relationship with the partner.11
AGW significantly decreased the sexual function of women compared to men. Decreased sexual function following AGW is more common in women because psychological factors highly associate with the sexual function in women. The oncogenic nature of the disease,12,13 pain during sexual intercourse, psychosocial problems such as: sense of helplessness, shame and questions about loyalty to the partner are other factors influencing the females’ sexual function after confirmed HPV infection.14,15
According to Woodhall et al. study, genital warts appeared to affect young women the most. This is in contrast to men between 16 to 19 years old, who did not appear to have a significant loss of quality of life in comparison to normal population. This finding might be due to the fact that stigma associated with STI is more severe in women than in men; however, more investigations are needed to evaluate this difference.16
A 6-month prospective study by Drolet et al.17 revealed that anogenital warts had a negative effect on the quality of life for both men and women. This impact was directly related to the duration of the disease and episodes of recurrence, and persisted as long as disease persisted. Among different aspects of quality of life, having anogenital warts had the greatest impact on sexual activity, self-image and self-esteem, and worries about partner and transmission of the disease.
Mortensen et al.18 found out that most of the patients reported that among different psychosexual aspects, mostly their sexuality and love life had damaged due to genital warts. Their libido was decreased and their desire to initiate sex was reduced and pleasure and satisfaction was lost during coitus. This is mostly due to fear of disease transmission or disgusting the partner, negative self-perception and dyspareunia due to treatment. These negative effects reduced the stability of relationships and for single patients, genital warts affected their desire to seek for a new partner. The study also revealed that some participants had negative feelings such as guilt or anger because they assumed that they did not protected themselves and their partners carefully.
Conversely, our results indicate that marital status did not considerably affect the ENRICH scale items in the case group. Confirming our results, a research by Newton et al. demonstrated that there was not any association between relationship status and significant differences in aspects of sexual self-concept in STD patients.19
Several limitations should be bear in mind when interpreting these findings. First, Cultural characteristics of Iranian society may indeed had affected our results. Traditionally prohibited premarital and extramarital sexual relationships empowered by religious political structures had restricted sex education which resulted in inadequate knowledge and negative attitude toward STIs.20 Presumably in a patriarchal society, Women are more vulnerable to suffer from social stigma and psychological ailments related to STIs. Yet as few studies had investigated different aspects of Iranian people's sexual life it is difficult to integrate this study's findings with local cultural factors in a clear evidence-based argument.
Second, patients who admitted to our educational clinic had more adverse effects and thus our samples may not be a representative of the whole AGW patients. Third, the impact of duration and recurrence of the disease were not considered in our study, which can be addressed in future researches.
In conclusion, based on presented evidence we recommend providing patients who suffer from AGW with a psychosexual education and consultation to improve their quality of life.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Nahidi M, Nahidi Y, Kardan G, Jarahi L, Aminzadeh B, Shojaei P, et al. Evaluación de la vida sexual y de la satisfacción matrimonial en pacientes con verruga anogenital. Actas Dermosifiliogr. 2019;110:522–526.



