



Plantar warts are caused by infection with human papillomavirus (HPV) types 1, 2, 4, or 57.1–3 Their treatment can be difficult when the lesion is located in a callused site subjected to significant pressure or when several warts are grouped together. Conventional treatments, which are usually destructive, cause pain and are not always effective. Therapy that does not result in scarring, which can remain painful for years, is recommended for plantar warts.
Imiquimod 5% cream is approved for the treatment of genital warts and has also been used successfully on viral warts in other sites.1,3,4 Moreover, there is scientific evidence supporting its efficacy and safety in the eradication of recalcitrant plantar warts without local adverse effects.1–3,5–7
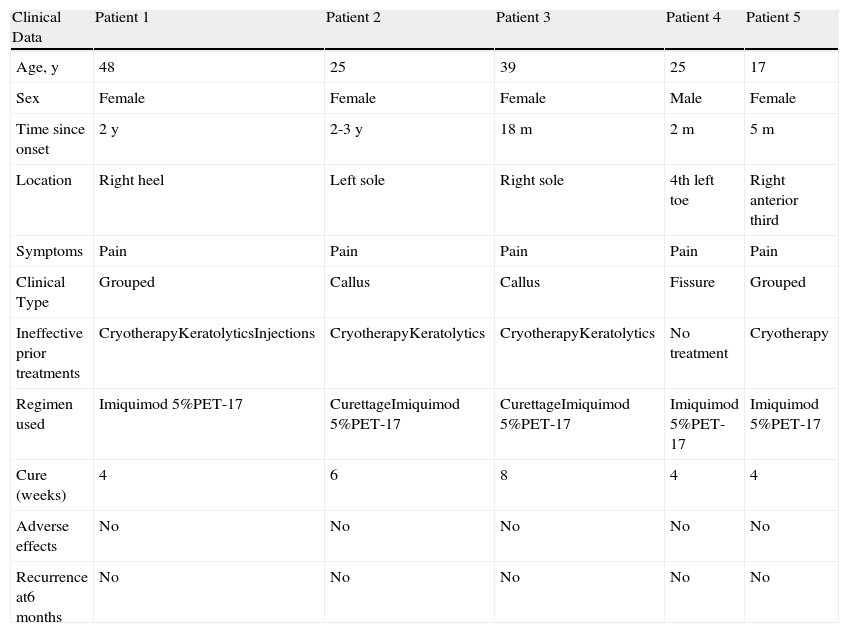
Table 1 shows the clinical characteristics of 5 patients who had painful plantar warts that made walking difficult. In 4 cases the warts had been resistant to other treatment, but they all responded very positively to imiquimod 5% cream (Figs. 1 and 2). In all cases, imiquimod was applied at night, without occlusion, 3 times a week, until the lesions disappeared. On days when imiquimod was not administered, petrolatum with 17% salicylic acid was applied. The hyperkeratosis associated with warts located in pressure zones was removed mechanically with a scalpel every 2 weeks (cases 2 and 3).
Clinical Data for 5 Patients.
| Clinical Data | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 |
| Age, y | 48 | 25 | 39 | 25 | 17 |
| Sex | Female | Female | Female | Male | Female |
| Time since onset | 2 y | 2-3 y | 18 m | 2 m | 5 m |
| Location | Right heel | Left sole | Right sole | 4th left toe | Right anterior third |
| Symptoms | Pain | Pain | Pain | Pain | Pain |
| Clinical Type | Grouped | Callus | Callus | Fissure | Grouped |
| Ineffective prior treatments | CryotherapyKeratolyticsInjections | CryotherapyKeratolytics | CryotherapyKeratolytics | No treatment | Cryotherapy |
| Regimen used | Imiquimod 5%PET-17 | CurettageImiquimod 5%PET-17 | CurettageImiquimod 5%PET-17 | Imiquimod 5%PET-17 | Imiquimod 5%PET-17 |
| Cure (weeks) | 4 | 6 | 8 | 4 | 4 |
| Adverse effects | No | No | No | No | No |
| Recurrence at6 months | No | No | No | No | No |
PET-17 Petrolatum with 17% salicylic acid.


Imiquimod (1-[2methypropyl]-1 H-imidazole [4,5c]quinolin-4amine) is an immune response modifier with antiviral and antitumor activity mediated by the induction of helper T (Th) 1 cytokines.8,9 The exact mechanism of action remains unclear, but activation of the immune system is thought to be responsible for eradicating the virus and curing the warts. This mechanism of action is highly advantageous in the treatment of viral plantar warts, compared with the more destructive traditional methods.10 Also recommended is the concomitant use of therapies, such as the application of salicylic petrolatum, cryotherapy, and peeling to eliminate the stratum corneum and facilitate drug absorption in these areas of more keratinized skin. The cream can also be applied under occlusion.1–3,6
Imiquimod therapy is less traumatic than ablative treatments, which often involve local tissue destruction and pain, and any local inflammatory reactions tend to be mild and transitory. As no adverse local or general reactions were reported in the cases reviewed in the literature or those presented in this study, imiquimod is well tolerated and therefore highly recommendable.
Imiquimod also stimulates immunological memory for HPV and, as a result, wart recurrence after treatment with this drug may be lower than with other therapies.9 Moreover, the cream can be applied by the patient at home, thus saving on time and repeated hospital visits.
Imiquimod has been successfully used to treat plantar warts in different regimens: daily application,1 on alternate days, 3 times a week,2 with or without occlusion.3,5 However, no single therapy has proven to be better than another. Nevertheless, all authors recommend combining imiquimod with keratolytic agents for plantar warts and mechanical removal of the stratum corneum in the case of warts associated with calluses and located on pressure points.1–3,6
Topical imiquimod is not the first-line treatment for plantar warts but can be surprisingly useful for extensive groups of warts, as in patients 1 and 5. It can also produce a beneficial synergistic effect when associated with previously inefficient procedures, as occurred in patients 2 and 3. The results obtained in these 5 patients provide clinical evidence of the therapeutic efficacy of imiquimod 5% cream in the treatment of recalcitrant plantar warts as reported by other authors.1,2,5–7 Patient tolerance and satisfaction were very high, and product efficacy was excellent, each patient only needing one box of imiquimod 5% cream and 2 or 3 hospital visits to solve a problem that had developed over many years and had resulted in very high direct and indirect costs.
Please cite this article as: López-Giménez MT. Tratamiento eficiente de 5 casos de verrugas plantares recalcitrantes con imiquimod 5%. Actas Dermosifiliogr. 2013;104:640–2.



