



A 40-year-old woman with no personal or family history of interest was seen for a mildly pruritic rash of progressive onset on both forearms that had appeared 2 years earlier. The lesions were not exacerbated by sun exposure and had not improved following treatment with either antihistamines or topical corticosteroids. Physical examination revealed multiple, slightly raised papules of 1 to 2mm in diameter on the ventral forearms. The papules were monomorphic with an erythematous-brownish coloration (Fig. 1A and B). The patient had no lesions in any other areas of the integument or mucous membranes. Hematoxylin-eosin staining showed an epithelial proliferation in the middle and upper reticular dermis consisting of ductal structures covered with a cuboidal epithelium. Some of the ductal structures had comma-shaped epithelial prolongations (Fig. 2). Mitosis and cellular atypia were absent. Culture for human papilloma virus was negative. Based on these clinical and histological findings the patient was diagnosed with multiple acral syringomas.

.")
Photoprotection and topical treatment with 0.05% tretinoin twice daily were prescribed. After 4 months of treatment the patient reported flattening of the lesions and a reduction in pruritus, and showed good tolerance to the treatment.
Syringoma is a common benign adnexal tumor derived from the intraepidermal portion of the eccrine excretory (acrosyringeal) duct. The most common presentation is small, yellowish or skin-colored papules on the lower eyelids of middle-aged women. Less frequent locations include the neck, thorax, armpits, and genital region.1
In 1987 Friedman and Butler2 proposed a classification system that distinguishes 4 clinical variants of syringoma: localized (solitary or multiple), familial, Down's syndrome-associated, and generalized (multiple or eruptive) forms. Eruptive syringoma can be associated with Nicolau-Balus syndrome, which is characterized by the presence of eruptive syringomas, milium cysts, and vermiculate atrophoderma.3
Histologically, syringoma is characterized by the proliferation of cells arranged in nests, cords, or tubular structures and located in the upper dermis. Depending on the plane of section, syringomas can have a comma- or tadpole-like morphology. The tubular structures exhibit ductal differentiation and an eosinophilic cuticle lining the lumen. Bundles of thick, sclerotic collagen are evident in the surrounding stroma. The histological differential diagnosis should include microcystic adnexal carcinoma, desmoplastic trichoepithelioma, sclerodermiform basal cell carcinoma, and sclerosing adenosis of the sweat glands. Syringoma is distinguished from microcystic adnexal carcinoma by its smaller size, greater symmetry, more superficial location in the dermis, and the absence of prominent horn cysts. While solid strands of basophilic epithelial cells and corneal cysts may be observed in desmoplastic trichoepithelioma, ductal structures are absent. Sclerodermiform basal cell carcinoma lacks ductal structures containing amorphous material. Finally, stellate sclerosis, which is absent in syringoma, is very common in the benign condition known as sclerosing adenosis of the sweat glands.4,5
Acral syringoma is limited to the distal areas of the upper and/or lower extremities. This form is very rare, and only a few cases are described in the literature (Table 1).6,7 Distinctive characteristics of this form include onset at more advanced ages and a similar prevalence in men and women.6,8 Concomitant periorbital involvement is absent in most reported cases. It is important to highlight the occasional association of acral syringoma with malignant tumors, including pulmonary carcinoid tumor, cutaneous melanoma, basal cell carcinoma, breast carcinoma, and promyelocytic leukemia.6–8 Our patient was a healthy woman with no symptoms and no known tumors.
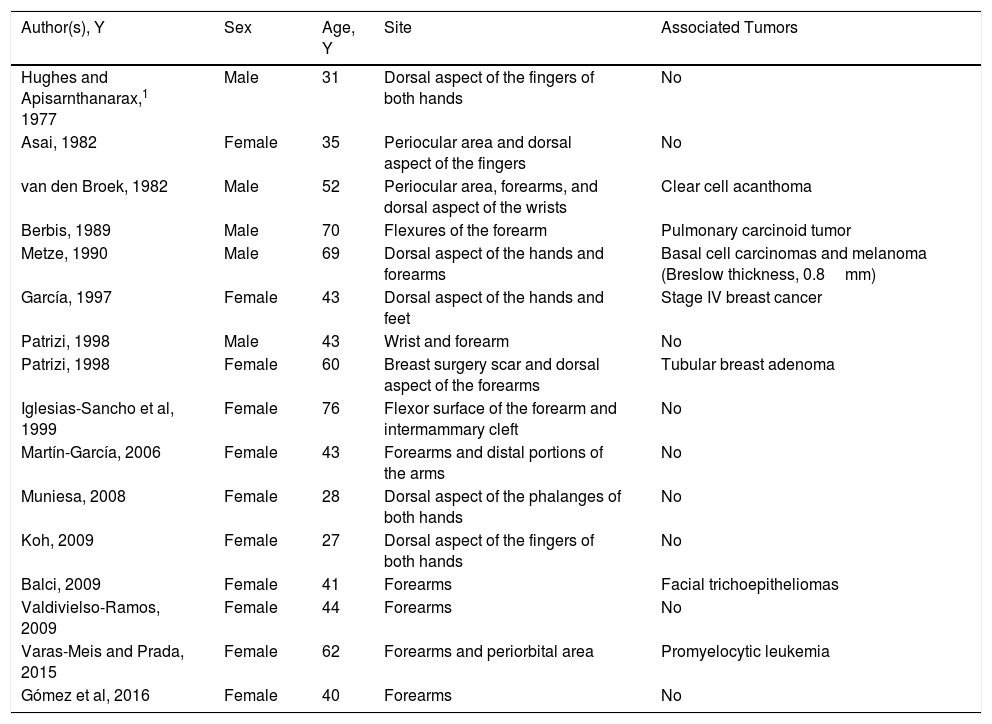
Published Cases of Acral Syringoma.
| Author(s), Y | Sex | Age, Y | Site | Associated Tumors |
|---|---|---|---|---|
| Hughes and Apisarnthanarax,1 1977 | Male | 31 | Dorsal aspect of the fingers of both hands | No |
| Asai, 1982 | Female | 35 | Periocular area and dorsal aspect of the fingers | No |
| van den Broek, 1982 | Male | 52 | Periocular area, forearms, and dorsal aspect of the wrists | Clear cell acanthoma |
| Berbis, 1989 | Male | 70 | Flexures of the forearm | Pulmonary carcinoid tumor |
| Metze, 1990 | Male | 69 | Dorsal aspect of the hands and forearms | Basal cell carcinomas and melanoma (Breslow thickness, 0.8mm) |
| García, 1997 | Female | 43 | Dorsal aspect of the hands and feet | Stage IV breast cancer |
| Patrizi, 1998 | Male | 43 | Wrist and forearm | No |
| Patrizi, 1998 | Female | 60 | Breast surgery scar and dorsal aspect of the forearms | Tubular breast adenoma |
| Iglesias-Sancho et al, 1999 | Female | 76 | Flexor surface of the forearm and intermammary cleft | No |
| Martín-García, 2006 | Female | 43 | Forearms and distal portions of the arms | No |
| Muniesa, 2008 | Female | 28 | Dorsal aspect of the phalanges of both hands | No |
| Koh, 2009 | Female | 27 | Dorsal aspect of the fingers of both hands | No |
| Balci, 2009 | Female | 41 | Forearms | Facial trichoepitheliomas |
| Valdivielso-Ramos, 2009 | Female | 44 | Forearms | No |
| Varas-Meis and Prada, 2015 | Female | 62 | Forearms and periorbital area | Promyelocytic leukemia |
| Gómez et al, 2016 | Female | 40 | Forearms | No |
Adapted from Valdivielso-Ramos et al.6
The differential diagnosis of papular acral lesions should include syringoma, as well as lichen planus, milium cysts, urticaria pigmentosa, flat warts, and certain photodermatoses.8,9
Given the benign nature of the process treatment is not required, although aesthetic or symptomatic treatment is often instituted. Available therapeutic options include surgical excision, electrocoagulation, cryotherapy, laser ablation, topical retinoids, and trichloroacetic acid.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Gómez-de Castro C, Vivanco Allende B, García-García B. Siringomas acrales múltiples. Actas Dermosifiliogr. 2018;109:834–836.



