

The treatment of inflammatory and autoimmune diseases is challenging because of their frequency and complexity. Treatment of these diseases is based on the suppression of the patient's immune system using corticosteroids, corticosteroid-sparing immunosuppressive agents, and biologic drugs, making an understanding of the management of immunosuppressive therapy essential. Before an immunosuppressive agent is prescribed, a study must be carried out to identify contraindications, detect latent infections, and determine the most appropriate dose. During treatment, regular monitoring is required to detect adverse effects. The clinician must be familiar with the time lag between start of treatment and onset of the immunosuppressive effect as well as the maximum recommended duration of treatment and cumulative dose for each drug. As dermatologists we are accustomed to using these immunosuppressive agents, but we should have a good knowledge of the guidelines for their use and the monitoring required in each case if we are to reduce variability and avoid potentially serious adverse effects.
Las enfermedades inflamatorias y autoinmunes constituyen un desafío terapéutico por frecuencia y complejidad. Su tratamiento se basa en la inmunosupresión del paciente con glucocorticoides, inmunosupresores ahorradores de corticoides y fármacos biológicos, siendo imprescindible por tanto conocer su manejo. Cuando se va a pautar un inmunosupresor es necesario realizar un estudio previo para detectar contraindicaciones, infecciones latentes o determinar la dosis más adecuada del fármaco. Durante el tratamiento se deben realizar controles periódicos para detectar efectos secundarios. Cada fármaco tiene un tiempo de inicio de acción que es preciso conocer, así como una duración o dosis acumulada máxima recomendada. Los dermatólogos estamos habituados al uso estos fármacos inmunosupresores, pero es necesario tener claras las pautas y los controles necesarios con cada uno, para disminuir la variabilidad y evitar efectos adversos potencialmente graves.
Dermatologic autoimmune or inflammatory diseases are usually managed with immunosuppressants. Care must be taken to find a point of balance that attenuates the abnormal inflammatory response while causing the least possible immunosuppression.
The prescriber must be aware of each immunosuppressant's unique time to onset of action, level of acute toxicity, and dosage regimens. An intense, rapid response is sometimes warranted, but a goal in other circumstances might be a treatment that can be followed over the long term.
This review deals with classic immunosuppressants. Neither glucocorticoids nor biologics will be discussed.
Pretreatment Tests and VaccinationsBefore suppressing a patient's immune response, information is required for ruling out contraindications, tailoring the dosage, and planning measures to reduce inherent risk.
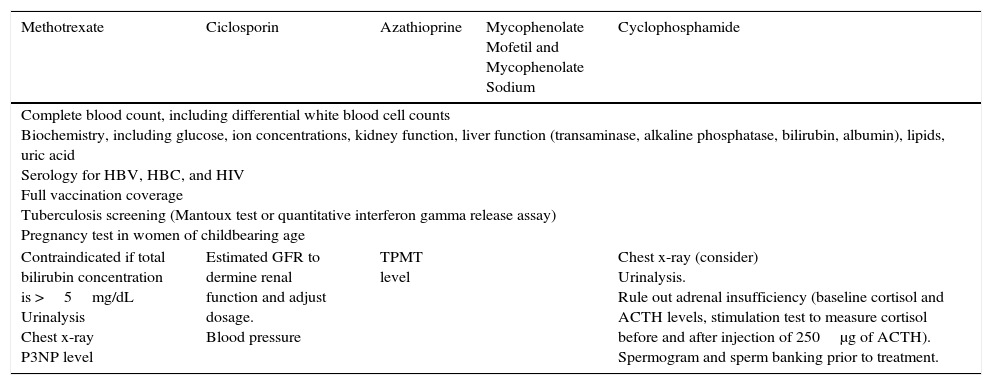
Certain laboratory tests are needed for prescribing any of these drugs, but particular immunosuppressants also have specific requirements1 (Table 1).
Complementary Tests to Order Before Starting Immunosuppressant Therapy.
| Methotrexate | Ciclosporin | Azathioprine | Mycophenolate Mofetil and Mycophenolate Sodium | Cyclophosphamide |
|---|---|---|---|---|
| Complete blood count, including differential white blood cell counts Biochemistry, including glucose, ion concentrations, kidney function, liver function (transaminase, alkaline phosphatase, bilirubin, albumin), lipids, uric acid Serology for HBV, HBC, and HIV Full vaccination coverage Tuberculosis screening (Mantoux test or quantitative interferon gamma release assay) Pregnancy test in women of childbearing age | ||||
| Contraindicated if total bilirubin concentration is >5mg/dL Urinalysis Chest x-ray P3NP level | Estimated GFR to dermine renal function and adjust dosage. Blood pressure | TPMT level | Chest x-ray (consider) Urinalysis. Rule out adrenal insufficiency (baseline cortisol and ACTH levels, stimulation test to measure cortisol before and after injection of 250μg of ACTH). Spermogram and sperm banking prior to treatment. | |
Abbreviations: ACTH, adrenocorticotropic hormone; GFR, glomerular filtration rate; HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; P3NP, procollagen type III N-terminal peptide; TPMT, thiopurine methyltransferase.
Because vaccination coverage should be on record for all patients, serology is included in the test battery.2–5 If the patient's clinical condition permits, required vaccinations or booster doses should be scheduled at least 2 weeks before immunosuppressant therapy starts. If vaccination is not feasible beforehand, it should not be undertaken until at least 3 months after treatment stops given that live virus vaccines carry the risk of infection, and immunization may not be achieved if inactivated viruses are used.
Vaccination against varicella should be tailored to the individual. If a pediatric vaccination schedule must be followed, immunosuppressants should be interrupted 2 weeks before vaccination and not restarted until 2 weeks afterwards.6
Two types of pneumococcal vaccines are available: the 23-valent polysaccharide (PPSV23) and 13-valent conjugate (PCV13) versions. Spanish health authorities stipulate a sequential vaccination schedule for patients on immunosuppressants.7 The schedule starts with a dose of PCV13 before treatment and is followed by a dose of PPSV23 at least 8 weeks later. If the patient is already under treatment, these criteria should be applied when the first consultation takes place. A booster dose of PPSV23 should be given at 5 years.
Patients on immunosuppressants should receive the same influenza vaccination produced for the general population every year.8
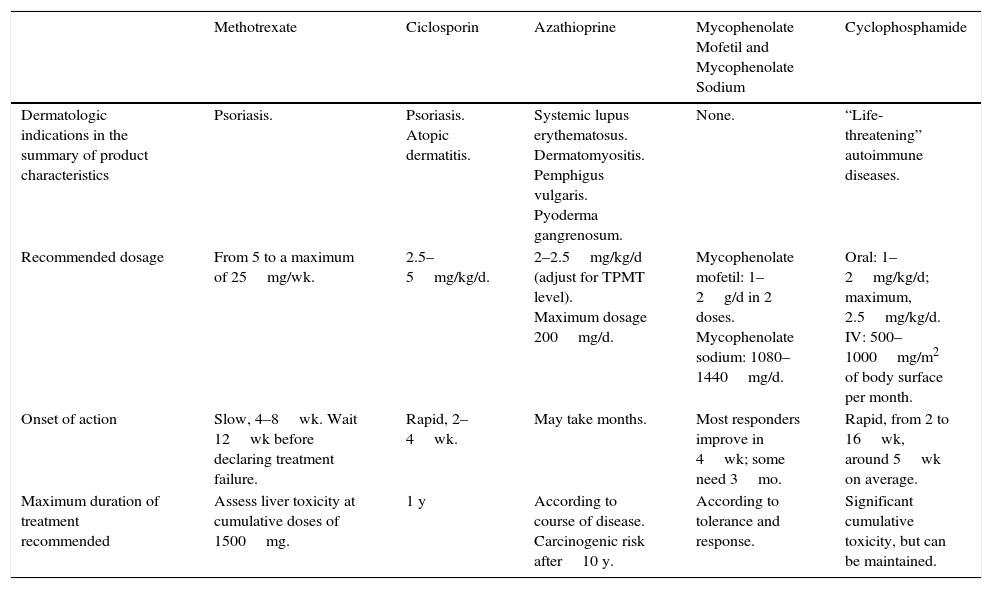
Certain factors affect the choice of one immunosuppressant drug (Table 2) over another:
- •
whether or not the patient has a medical history that includes a contraindication for a particular immunosuppressant or new testing reveals such a contraindication,
- •
whether or not the drug's summary of product characteristics includes the patient's disease,9–13
- •
whether or not an intense, rapid response is required,
- •
or alternatively, whether the prescriber seeks a maintenance of effect over a long course of treatment.
Basic Features of Immunosuppressants to Know When Selecting a Therapy.
| Methotrexate | Ciclosporin | Azathioprine | Mycophenolate Mofetil and Mycophenolate Sodium | Cyclophosphamide | |
|---|---|---|---|---|---|
| Dermatologic indications in the summary of product characteristics | Psoriasis. | Psoriasis. Atopic dermatitis. | Systemic lupus erythematosus. Dermatomyositis. Pemphigus vulgaris. Pyoderma gangrenosum. | None. | “Life-threatening” autoimmune diseases. |
| Recommended dosage | From 5 to a maximum of 25mg/wk. | 2.5–5mg/kg/d. | 2–2.5mg/kg/d (adjust for TPMT level). Maximum dosage 200mg/d. | Mycophenolate mofetil: 1–2g/d in 2 doses. Mycophenolate sodium: 1080–1440mg/d. | Oral: 1–2mg/kg/d; maximum, 2.5mg/kg/d. IV: 500–1000mg/m2 of body surface per month. |
| Onset of action | Slow, 4–8wk. Wait 12wk before declaring treatment failure. | Rapid, 2–4wk. | May take months. | Most responders improve in 4wk; some need 3mo. | Rapid, from 2 to 16wk, around 5wk on average. |
| Maximum duration of treatment recommended | Assess liver toxicity at cumulative doses of 1500mg. | 1 y | According to course of disease. Carcinogenic risk after10 y. | According to tolerance and response. | Significant cumulative toxicity, but can be maintained. |
Abbreviations: IV, intravenous; TPMT, thiopurine methyltransferase.
Source: Summaries of product characteristics posted by the Spanish Agency for Medicines and Health Products. Available from https://www.aemps.gob.es/cima/fichasTecnicas.do?metodo=detalleForm
Once an immunosuppressant is selected, it must be fully understood if we are to achieve the best results for our patient. For practical purposes we will analyze the main aspects relevant to managing the immunosuppressants most often prescribed by dermatologists (Tables 3–7).
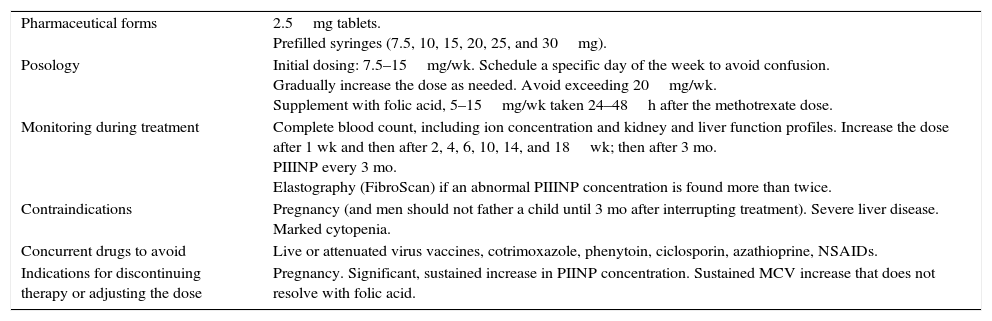
Practical Aspects of Treatment With Methotrexate.
| Pharmaceutical forms | 2.5mg tablets. Prefilled syringes (7.5, 10, 15, 20, 25, and 30mg). |
| Posology | Initial dosing: 7.5–15mg/wk. Schedule a specific day of the week to avoid confusion. Gradually increase the dose as needed. Avoid exceeding 20mg/wk. Supplement with folic acid, 5–15mg/wk taken 24–48h after the methotrexate dose. |
| Monitoring during treatment | Complete blood count, including ion concentration and kidney and liver function profiles. Increase the dose after 1 wk and then after 2, 4, 6, 10, 14, and 18wk; then after 3 mo. PIIINP every 3 mo. Elastography (FibroScan) if an abnormal PIIINP concentration is found more than twice. |
| Contraindications | Pregnancy (and men should not father a child until 3 mo after interrupting treatment). Severe liver disease. Marked cytopenia. |
| Concurrent drugs to avoid | Live or attenuated virus vaccines, cotrimoxazole, phenytoin, ciclosporin, azathioprine, NSAIDs. |
| Indications for discontinuing therapy or adjusting the dose | Pregnancy. Significant, sustained increase in PIINP concentration. Sustained MCV increase that does not resolve with folic acid. |
Abbreviations: MCV, mean corpuscular volume; NSAID, nonsteroidal anti-inflammatory drug; PIIINP, procollagen type III N-terminal peptide.
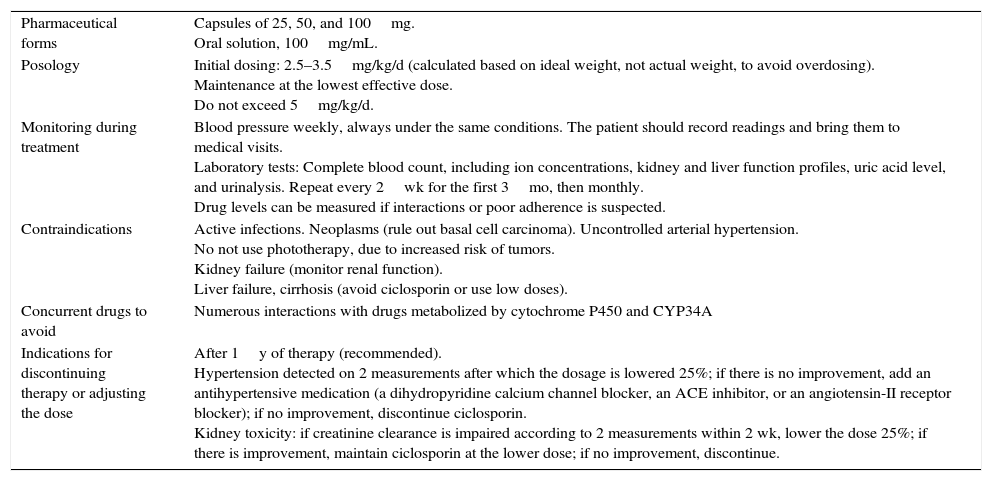
Practical Aspects of Treatment With Ciclosporin.
| Pharmaceutical forms | Capsules of 25, 50, and 100mg. Oral solution, 100mg/mL. |
| Posology | Initial dosing: 2.5–3.5mg/kg/d (calculated based on ideal weight, not actual weight, to avoid overdosing). Maintenance at the lowest effective dose. Do not exceed 5mg/kg/d. |
| Monitoring during treatment | Blood pressure weekly, always under the same conditions. The patient should record readings and bring them to medical visits. Laboratory tests: Complete blood count, including ion concentrations, kidney and liver function profiles, uric acid level, and urinalysis. Repeat every 2wk for the first 3mo, then monthly. Drug levels can be measured if interactions or poor adherence is suspected. |
| Contraindications | Active infections. Neoplasms (rule out basal cell carcinoma). Uncontrolled arterial hypertension. No not use phototherapy, due to increased risk of tumors. Kidney failure (monitor renal function). Liver failure, cirrhosis (avoid ciclosporin or use low doses). |
| Concurrent drugs to avoid | Numerous interactions with drugs metabolized by cytochrome P450 and CYP34A |
| Indications for discontinuing therapy or adjusting the dose | After 1y of therapy (recommended). Hypertension detected on 2 measurements after which the dosage is lowered 25%; if there is no improvement, add an antihypertensive medication (a dihydropyridine calcium channel blocker, an ACE inhibitor, or an angiotensin-II receptor blocker); if no improvement, discontinue ciclosporin. Kidney toxicity: if creatinine clearance is impaired according to 2 measurements within 2 wk, lower the dose 25%; if there is improvement, maintain ciclosporin at the lower dose; if no improvement, discontinue. |
Abbreviations: ACE, angiotensin converting enzyme.
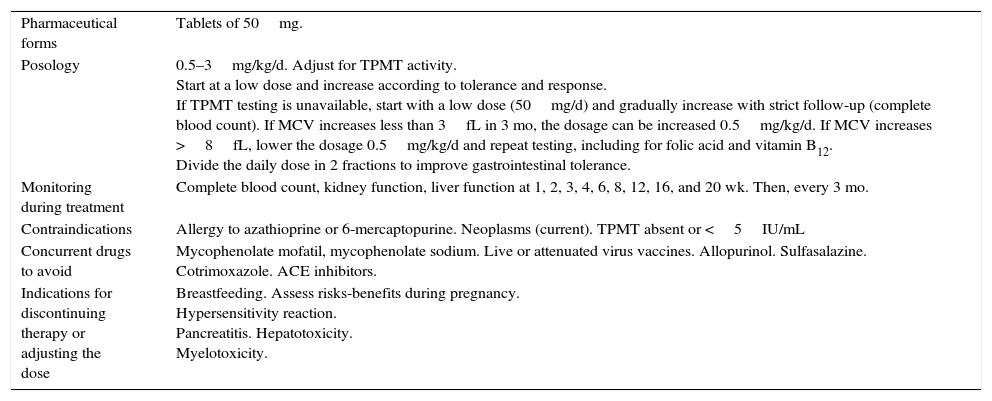
Practical Aspects of Treatment With Azathioprine.
| Pharmaceutical forms | Tablets of 50mg. |
| Posology | 0.5–3mg/kg/d. Adjust for TPMT activity. Start at a low dose and increase according to tolerance and response. If TPMT testing is unavailable, start with a low dose (50mg/d) and gradually increase with strict follow-up (complete blood count). If MCV increases less than 3fL in 3 mo, the dosage can be increased 0.5mg/kg/d. If MCV increases >8fL, lower the dosage 0.5mg/kg/d and repeat testing, including for folic acid and vitamin B12. Divide the daily dose in 2 fractions to improve gastrointestinal tolerance. |
| Monitoring during treatment | Complete blood count, kidney function, liver function at 1, 2, 3, 4, 6, 8, 12, 16, and 20 wk. Then, every 3 mo. |
| Contraindications | Allergy to azathioprine or 6-mercaptopurine. Neoplasms (current). TPMT absent or <5IU/mL |
| Concurrent drugs to avoid | Mycophenolate mofatil, mycophenolate sodium. Live or attenuated virus vaccines. Allopurinol. Sulfasalazine. Cotrimoxazole. ACE inhibitors. |
| Indications for discontinuing therapy or adjusting the dose | Breastfeeding. Assess risks-benefits during pregnancy. Hypersensitivity reaction. Pancreatitis. Hepatotoxicity. Myelotoxicity. |
Abbreviations: ACE, angiotensin converting enzyme; MCV, mean corpuscular volume; TPMT, thiopurine methyltransferase.
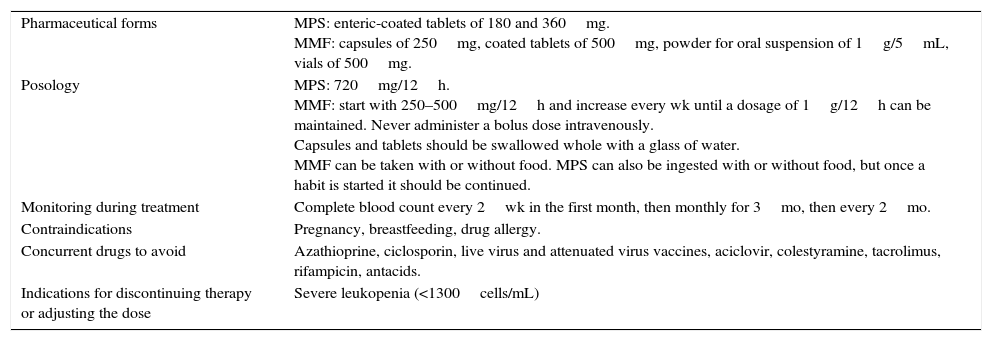
Practical Aspects of Treatment With Mycophenolate Mofetil and Mycophenolate Sodium.
| Pharmaceutical forms | MPS: enteric-coated tablets of 180 and 360mg. MMF: capsules of 250mg, coated tablets of 500mg, powder for oral suspension of 1g/5mL, vials of 500mg. |
| Posology | MPS: 720mg/12h. MMF: start with 250–500mg/12h and increase every wk until a dosage of 1g/12h can be maintained. Never administer a bolus dose intravenously. Capsules and tablets should be swallowed whole with a glass of water. MMF can be taken with or without food. MPS can also be ingested with or without food, but once a habit is started it should be continued. |
| Monitoring during treatment | Complete blood count every 2wk in the first month, then monthly for 3mo, then every 2mo. |
| Contraindications | Pregnancy, breastfeeding, drug allergy. |
| Concurrent drugs to avoid | Azathioprine, ciclosporin, live virus and attenuated virus vaccines, aciclovir, colestyramine, tacrolimus, rifampicin, antacids. |
| Indications for discontinuing therapy or adjusting the dose | Severe leukopenia (<1300cells/mL) |
Abbreviations: MMF, mycophenolate mofetil; MPS, mycophenolate sodium.
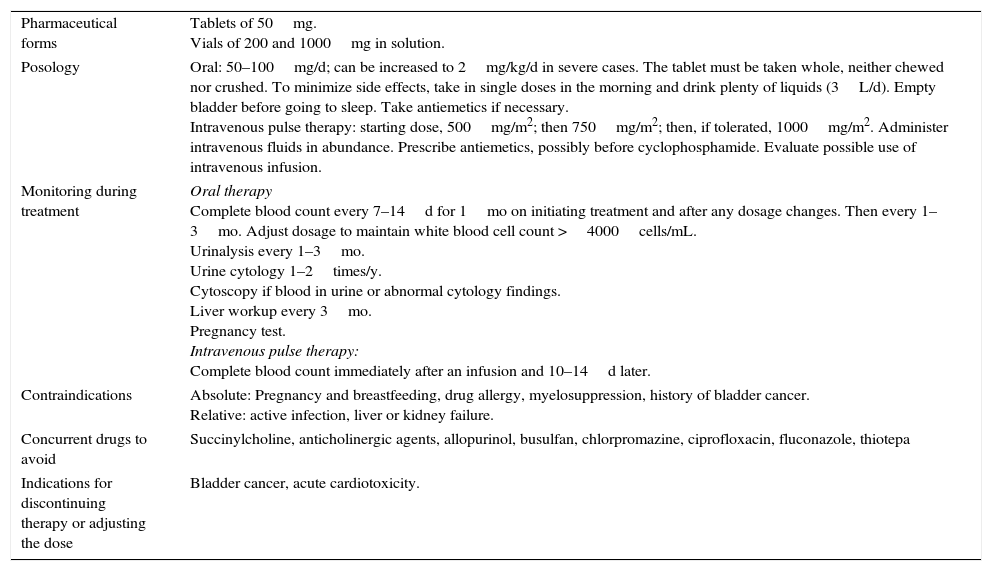
Practical Aspects of Treatment With Cyclophosphamide.
| Pharmaceutical forms | Tablets of 50mg. Vials of 200 and 1000mg in solution. |
| Posology | Oral: 50–100mg/d; can be increased to 2mg/kg/d in severe cases. The tablet must be taken whole, neither chewed nor crushed. To minimize side effects, take in single doses in the morning and drink plenty of liquids (3L/d). Empty bladder before going to sleep. Take antiemetics if necessary. Intravenous pulse therapy: starting dose, 500mg/m2; then 750mg/m2; then, if tolerated, 1000mg/m2. Administer intravenous fluids in abundance. Prescribe antiemetics, possibly before cyclophosphamide. Evaluate possible use of intravenous infusion. |
| Monitoring during treatment | Oral therapy Complete blood count every 7–14d for 1mo on initiating treatment and after any dosage changes. Then every 1–3mo. Adjust dosage to maintain white blood cell count >4000cells/mL. Urinalysis every 1–3mo. Urine cytology 1–2times/y. Cytoscopy if blood in urine or abnormal cytology findings. Liver workup every 3mo. Pregnancy test. Intravenous pulse therapy: Complete blood count immediately after an infusion and 10–14d later. |
| Contraindications | Absolute: Pregnancy and breastfeeding, drug allergy, myelosuppression, history of bladder cancer. Relative: active infection, liver or kidney failure. |
| Concurrent drugs to avoid | Succinylcholine, anticholinergic agents, allopurinol, busulfan, chlorpromazine, ciprofloxacin, fluconazole, thiotepa |
| Indications for discontinuing therapy or adjusting the dose | Bladder cancer, acute cardiotoxicity. |
Methotrexate, an antimetabolite analog of folic acid, inhibits dihydrofolate reductase. It is unquestionably one of the most often prescribed immunosuppressants in dermatology.14
Although psoriasis is the only indication listed in the product summary,13,15,16 many studies have supported this drug's use in other conditions.17 Some examples are autoimmune bullous diseases18; severe adult atopic dermatitis19; alopecia areata20; chronic urticaria21; cutaneous lupus erythematosus22,23; sarcoidosis, scleroderma, lymphomatoid papulosis and other lymphoproliferative disorders17,24; and keratoacanthomas.25
Methotrexate is available in tablets of 2.5mg and syringes prefilled with doses ranging from 7.5 to 30mg (Table 3). Oral administration is much more economical than parenteral injection and the bioequivalence is similar, at least up to a weekly dose of 17.5mg.14,16 However, gastrointestinal symptoms are common with oral intake, and injections are therefore recommended when the dose exceeds 15mg to prevent digestive intolerance. Parenteral administration is also advisable when the patient is at risk of confusing doses or adherence is poor.26
The patient must be told that the drug is taken or injected once a week, not daily, if serious side effects are to be avoided.17,26 It is good practice to establish a particular time each week that takes into consideration that the dose will be followed by days of discomfort and that samples for laboratory tests must be collected the day before dosing, as long as possible before the drug is actually taken. The entire oral dose can be ingested at once or in 2 or 3 fractions separated by 12hours.15
A test dose is not currently considered necessary.27 A starting dosage of 7.5 to 15mg/wk should be given and gradually increased until the response is satisfactory. Increases of 2.5 to 5mg can be tried every 4 to 6 weeks.17,19 Responders usually improve at 4weeks, but we have waited up to 12weeks before deciding that treatment has failed. A regimen of 15mg/wk is usually effective. The approach should be reviewed if 25mg/wk is exceeded.26
The strategy to follow is similar in psoriasis and other diseases. In autoimmune bullous diseases, for example, certain patients are nonresponders (13% in pemphigus vulgaris, 4% in bullous pemphigoid), and no data on predictors of failure are available. On the other hand, mortality due to serious infection is considerable (3.7% in pemphigus vulgaris, 2.5% in bullous pemphigoid). Nonetheless methotrexate therapy remains a good corticosteroid-sparing strategy.18
Methotrexate should be accompanied by folic or folinic acid supplementation, which significantly reduces adverse effects on the liver and nonsignificantly improves effects on mucosal, gastrointestinal and blood tissues but does not prevent the development of pulmonary fibrosis.26,28 Some studies consider supplementation to be contraindicated in the interest of efficacy, but a reduction in methotrexate's effect with folic acid is fairly unlikely28 because the 2 drugs promote the anti-inflammatory action of adenosine through different mechanisms.16 Folic acid and folinic acid do not appear to differ in effectiveness, and the former is less costly. Dosage regimens are debated. They vary from 5 to 30mg/wk unless other conditions requiring folic or folinic acid supplementation are present, in which case 5mg/week taken 24 to 48hours after the methotrexate dose should be sufficient.26
One of the main adverse effects of methotrexate is liver fibrosis. One systematic review found that the risk for fibrosis increased 22% in patients with methotrexate-treated psoriasis; however, risk was not significantly related to duration of therapy or cumulative dose.29 The authors therefore concluded that fibrosis develops only in a certain subgroup of patients whose characteristics could not be determined due to the low quality of evidence provided by the studies reviewed. It is likely that comorbid conditions such as obesity or alcohol intake exacerbate risk in some. A noninvasive means for detecting fibrosis without resorting to liver biopsy is required. The most widely studied approaches are the measurement of biomarkers (eg, procollagen type III N-terminal peptide30) and the use of imaging techniques such as elastography (eg, FibroScan). One meta-analysis showed that these 2 techniques applied individually have low discriminatory power in screening.31 However, combining various biomarkers (eg, in the enhanced liver fibrosis panel) or biomarkers and imaging may be more useful.
CiclosporinCiclosporin is a calcineurin inhibitor that acts on T cells.The summary of product characteristics for this drug lists psoriasis and atopic dermatitis as the dermatologic indications. However, ciclosporin has been used to effectively treat Stevens–Johnson syndrome,32 lichen planus and lichen planopilaris,33 pyoderma gangrenosum, chronic urticaria, autoimmune blistering diseases, suppurative hidradenitis, and more.34,35
The great advantage of ciclosporin is its rapid onset of action. Good control of disease can be achieved in a few months with a short treatment cycle.
Dose regimens range from 2.5 to 5mg/kg/d36 (Table 4). Although ciclosporin is lipophilic, it is important to remember that distribution is mainly through lean tissues. Therefore, when the real weight of obese patients is used to calculate the dosage, the concentration of the circulating drug will be elevated and there is risk of toxicity. Consequently, the dose should be calculated based on the patient's ideal weight.37
The daily dose is usually divided into 2 fractions. Taking ciclosporin before food intake has been shown to facilitate absorption, allow for lower doses and favor more even, predictable pharmacokinetics. Ciclosporin should therefore be taken before breakfast and before the evening meal.38
It is generally not recommended to prolong treatment beyond 1 year because long treatment cycles carry greater risk of toxicity. However, strategies that allow treatment to be maintained as long as possible have been explored. The 2 usual approaches, particularly in psoriasis, involve rotations and combinations that allow for lower daily doses. Weekend pulse therapy is another possibility once a conventional regimen has acheived control of disease. This regimen consists of prescribing a maintenance dose of up to 5mg/kg/d for 2 consecutive days per week and resting for the rest of the week. In psoriasis the efficacy of this strategy is similar to that of continuous therapy even though the mean daily dose is significantly lower.39 This regimen has produced promising results in pediatric patients with severe atopic dermatitis, enabling long-term therapy that avoids relapses40 with less toxicity and a lower cumulative dose.
Two of the main adverse effects that require dosage adjustment are kidney damage and arterial hypertension. If the creatinine level increases 30% over baseline on 2 consecutive reports 2 weeks apart, the dose should be lowered 25%. Hypertension would indicate the same dose adjustment. If the creatinine level or blood pressure returns to normal, ciclosporin treatment can continue at the lower dose. However, if these 2 variables remain elevated or continue to rise after 4 weeks on the lower dose of ciclosporin, the drug should be discontinued.36,37
Ciclosporin treatment can generally be suspended immediately without a rebound effect, although gradual weaning can lengthen the period of resolution before the next flare-up. Indications for discontinuing treatment are the failure to achieve good control of disease by 12 weeks, the development of severe adverse effects (neoplasms, infections), or a failure of blood pressure or creatinine levels to return to normal after a dose reduction. Cyclosporin should ideally be halted during pregnancy, unless symptoms make treatment necessary and there are no safer alternatives. In case treatment continues, the pregnancy should be considered high risk and followed closely. Treatment interruptions may be necessary in children so that vaccinations can be scheduled.
AzathioprineAzathioprine is indicated for inflammatory diseases and the prevention of solid organ transplant rejection. This prodrug is promptly metabolized to 6-mercaptopurine, which is activated along various metabolic pathways by enzymes that form thioguanine nucleotides that are then incorporated into DNA, accounting for the drug's biological effects.41,42
Thiopurine methyltransferase (TPMT) is an enzyme that methylates various intermediate products, many of them inactive. In a small population percentage (0.3%) of individuals who are homozygous for one of the alleles associated with low or no activity, azathioprine would be contraindicated; in the 9% to 11% of heterozygotic individuals, activity is intermediate; finally, 89% to 91% of the population are homozygotic for an allele associated with high activity.41,43–45 Patients with high TPMT activity require higher doses of azathioprine to reach therapeutic levels than those with lower TPMT activity. However, low TPMT activity carries a higher risk of myelosuppression under treatment. Measurement of TPMT has been shown to be useful for establishing the safest and most effective dosage for each patient in both adults and children.43,46–48 Tests for TPMT are used increasingly often, and their cost has become more competitive. However, if testing is unavailable, azathioprine therapy can begin with low doses that are increased gradually under strict monitoring to detect early markers of myelosuppression.
Other adverse effects, whether idiosyncratic or dose dependent, bear no relation to TPMT activity and may appear even when enzyme levels remain normal.41,47,49,50 There has even been a reported case of treated alopecia areata in which bone marrow suppression developed in the context of normal TPMT concentrations.51 A recent meta-analysis identified a significant association between the presence of TPMT gene polymorphisms and general adverse effects of azathioprine therapy, bone marrow toxicity and gastric intolerance, although no association with hepatotoxicity was found.52
The measurement and genotyping of glutathione-S-transferase have proven useful for assessing the risk of leukopenia in patients with inflammatory bowel disease, especially in oriental populations; however, it remains to be determined whether this marker is related to any other adverse effects of azathioprine therapy.53
Patients mainly complain of bowel discomfort, with nausea, vomiting, diarrhea or abdominal pain, and these symptoms are the usual reason for discontinuing treatment. To avoid these adverse effects, doses can be fractioned and taken with food.45
If gastrointestinal discomfort is severe or prolonged, hepatotoxicity, hypersensitivity, and pancreatitis must be ruled out.50 In pancreatitis, symptoms and laboratory results usually improve rapidly when the drug is discontinued.
The carcinogenic potential of azathioprine therapy is one of the greatest concerns. The risk is difficult to calculate and varies greatly between patient series. In addition to immunosuppression, azathioprine itself has been shown to cause photosensitivity, specifically in the UV-A spectrum; sun exposure therefore has a synergistic carcinogenic effect in azathioprine-treated patients.42 Additional risk factors for developing skin cancer in these patients are prolonged treatment, high-dose regimens, and a fair-skinned phototype.50 In addition to skin cancer, there is risk of lymphoma, and cases of Kaposi's angiosarcoma and renal cell carcinoma have been described.54
Hypersensitivity to azathioprine can cause a variety of symptoms: fever, joint and muscle pain, nausea, hepatitis, interstitial nephritis, kidney failure, maculopapular rash, and panniculitis. A diagnostic challenge test can trigger a severe reaction, so it should be done in a hospital where the means for cardiopulmonary resuscitation are at hand. In such cases, 6-mercaptopurine therapy would be a better tolerated alternative.41
The risk of infection also increases. Viral warts, molluscum contagiosum, folliculitis, and impetigo are common in treated children.55
Mycophenolate Mofetil and Mycophenolate Sodium SaltThe selective, reversible inhibition of inosine monophosphate dehydrogenase type 2 by mycophenolate mofetil (MMF) or mycophenolate sodium (MPS) interferes with the purine synthesis pathway of T and B cells, but not other cells.56,57 MMF is a prodrug that becomes mycophenolic acid once digested. The MPS salt is sold in an enteric-coated form.58
MMF or MPS therapy is indicated in heart, liver, or kidney transplanted patients to prevent acute rejection. No approved dermatologic uses are listed in the product summaries.12
However, the use of these drugs has been explored in various inflammatory diseases because liver and kidney toxicity is higher with alternative immunosuppressants.
Onset of action, which is slower than in glucocorticoid or ciclosporin treatment, takes at least 1 month and sometimes 3 to 4 months. This therapeutic option, therefore, is for maintenance of effect,58 either by itself or as a corticosteroid-sparing strategy.
Good outcomes have been reported in pyoderma gangrenosum58 and severe atopic dermatitis with both MMF56 and MPS59,60 in both adults and children.61 Positive results have also been reported in pemphigus vulgaris,62 collagenosis,63,64 chronic idiopathic urticaria,65 and lichen planus and sarcoidosis.64 The results in psoriasis have been less positive,66 although one randomized clinical trial found that efficacy was statistically similar to that of methotrexate.67 Evidence generally comes from single case reports or case series. Hardly any high quality randomized clinical trials have been published.
Immunosuppressant doses of these drugs vary in inflammatory diseases; doses of 500mg to 1g of MMF are given every 12hours (or 720mg of MPS every 12 hours). If a daily dose of 2g of MMF is reached without response, plasma levels of mycophenolic acid should be measured to rule out poor adherence or decide whether to increase the dose if absorption is low.68 Plasma levels vary greatly between patients and, curiously, between diseases. Mycophenolic acid plasma trough level has been shown to be a poor predictor of the effectiveness and safety of MMF therapy.
A great advantage of MMF over other immunosuppressants is its good tolerance and safety profile, particularly with regard to renal toxicity, hepatotoxicity, and neurotoxicity.
The most commonly reported adverse effects (in 12%–36%) involve the digestive system63 and include diarrhea, nausea, vomiting, abdominal pain, and soft stools. These effects are dose dependent and rarely oblige discontinuance of treatment. Transaminase levels rise in some patients, but no clinical impact or clear hepatotoxicity has been reported. Enteric-coated MPS is better tolerated.
Leukopenia is observed more often than anemia or thrombocytopenia, and again, the relationship is dose dependant. At dosages of 3g/d, this adverse effect develops in 34% of patients.64 If neutrophil counts fall below 1300 cells/mL, discontinuance is indicated. Red cell dysplasia has been reported, particularly in transplanted patients.68 These hematologic effects usually improve quickly when the drug is discontinued or the dose is reduced.
Urinary tract symptoms (dysuria, urgency, frequent urination, sterile pyuria, or hematuria) are not unusual, especially at the beginning of treatment. They usually improve after a year.
Conclusions about the risk of infection and neoplasia vary greatly in the literature. Published studies are difficult to compare, given that transplanted patients tend to receive higher doses and take more concurrent immunosuppressants than patients who have inflammatory diseases.
CyclophosphamideCyclophosphamide is an alkylating agent that interferes with DNA replication by attaching an alkyl group to the guanine base,69 causing cell death. The drug targets T cells and, to a lesser degree, B cells.70 The usual oral dosage is 1 to 2mg/kg/d; the intravenous dosage is 500–1000mg/m2 of body surface every month.
Because this potent drug has adverse effects, it is reserved for particularly severe cases. Dermatologic indications are autoimmune bullous diseases (especially pemphigus vulgaris and pemphigus foliaceous), autoimmune systemic vasculitis; severe cutaneous lupus erythematosus; cutaneous manifestations of systemic sclerosis; and cutaneous T-cell lymphoma.71,72
A higher cumulative daily dose increases the risk of toxicity in oral administration. Therefore, different therapeutic regimens have attempted to minimize that risk. Among the strategies tried are monthly intravenous infusions either alone or combined with low-dose oral therapy, and a single immunoablative high dose without stem-cell rescue. The efficacy of these alternative approaches seems to differ little from that of daily oral doses.70–76 Intravenous pulse therapy, however, leads to a lower cumulative dose and seems to be safer.77
Digestive symptoms such as nausea, vomiting, diarrhea, and stomatitis are common. Nausea is reported more in pulse therapy than oral treatment. Antiemetic prophylaxis is recommended.
Myelosuppression is an acute, dose-dependent adverse effect that usually presents with leukopenia. Monitoring is required to adjust the dose to keep the white blood cell count above 3500 to 4000 cells/mL. If the neutrophil count falls to dangerously low levels, granulocytic-colony-stimulating factors may have to be given.77 Treatment with cotrimoxazole or dapsone is recommended to guard against Pneumocystis jirovecii infection.73 Between 9% and 15% of patients had to be hospitalized for severe herpes zoster infection in some series.71 As in the context of other immunosuppressant therapies, pneumococcus as well as regular influenza vaccinations are indicated.
Hemorrhagic cystitis is a typical side effect of cyclophosphamide therapy. The incidence ranges from 8% to 41%, depending on dose, and oral intake seems to be associated with greater risk than pulse treatments. This complication seems to be caused by urinary secretion of a metabolite (acrolein) that irritates the urothelium. Preventive measures include drinking plenty of liquids, not taking the drug at night, and voiding the bladder before going to bed so that acrolein does not remain in contact with the mucosal tissue all night. Intravenous pulse infusion should be accompanied by intense fluid therapy to force diuresis. Adjuvant treatment with sodium 2-mercaptoethane sulfonate (Mesna), which binds to and deactivates acrolein, is also an option. This drug is given immediately after and again 4 and 8hours after cyclophosphamide, and each infusion should contain a dose that is 20% of the cyclophosphamide dose. In other words, after a dose of 1000mg of cyclophosphamide, the patient should receive 3 doses containing 200mg of Mesna each.
The other adverse effects of cyclophosphamide involve gonadal toxicity. Oral intake in particular seems to lead to premature ovarian failure, azoospermia, menstrual irregularity, and potentially irreversible infertility. The use of testosterone in men and gonadotropin-releasing hormone analogs in women is a subject of debate. Cyclophosphamide should therefore be avoided in patients of reproductive age. If it must be prescribed, the patient should be referred for reproductive counseling to assess the advisability of cryopreservation.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Leis-Dosil V, Prats-Caelles I. Practical Management of Immunosuppressants in Dermatology. Actas Dermosifiliogr. 2018;109:24–34.



