


Epidemiological studies have shown that patients with psoriasis have a higher risk of developing certain metabolic disorders, particularly obesity. Psoriasis and obesity are linked through a common pathophysiological mechanism of chronic low-grade inflammation. Not only is obesity associated with a higher incidence of psoriasis and greater severity, but it also affects response to treatment. The dermatologic management of these patients must therefore take their overall metabolic situation into consideration. We present a review of the recent literature on this subject and practical recommendations on the management of this group of patients, including relevant additional tests and advice on diet and a healthy lifestyle.
A través de estudios epidemiológicos se ha identificado un mayor riesgo de desarrollar algunas alteraciones metabólicas en los pacientes con psoriasis, dentro de las cuales destaca la obesidad. La obesidad y la psoriasis estarían vinculadas mediante un mecanismo fisiopatológico común, que se explica por una inflamación crónica de bajo grado. No sólo la obesidad se asocia con una mayor incidencia y severidad de la psoriasis, sino que también afecta su respuesta al tratamiento. Como consecuencia, la aproximación dermatológica hacia estos pacientes debiera contemplar su condición metabólica global. Se presenta una revisión actual de la literatura con respecto a este nuevo tema, así como recomendaciones prácticas para ser consideradas en este grupo de pacientes, tales como exámenes complementarios, consejo nutricional y de hábitos de estilo de vida saludables.
It has recently been found that patients with psoriasis have a higher prevalence of certain metabolic disorders considered to be cardiovascular risk factors,1 particularly obesity, diabetes or impaired glucose tolerance, dyslipidemias, and systemic hypertension, which together are known as the metabolic syndrome.2 Psoriasis is now also considered to be a marker of increased risk of myocardial infarction in young patients.3
Obesity is a chronic disease characterized by excess weight due to increased energy deposits in the form of fat. Specifically, this excess weight due to an increase in body fat mass is described in relation to the height of the patient, and the diagnosis of overweight is established using the body mass index (BMI), defined as the weight in kilograms divided by the square of the height in meters. The World Health Organization4 currently recommends classification of the adult population into the following categories according to BMI cutoff points: normal, 18.5 to 24.9 kg/m2; overweight, 25 to 29.9kg/m2; and obese, greater than 30kg/m2.
Obesity is a growing epidemic worldwide.5 Both overweight and obesity have increased in Spain in recent years.6 The close association between obesity and higher mortality, as well as the increased risk of developing type 2 diabetes, systemic hypertension, dyslipidemia, cardiovascular disease, and cancer, among other diseases, makes obesity a major public health problem.6
The association between obesity and certain skin diseases has been extensively studied and demonstrated7,8; in the case of psoriasis, it was first detected in epidemiological studies conducted in Europe.9,10 In 1986, a Scandinavian study revealed a higher prevalence of obesity in women with psoriasis than in other women.10 Later, Herron11 provided further evidence of this association when he detected a higher probability of developing obesity in his cohort of 500 patients with psoriasis than in the rest of the population of the state of Utah, United States (34% vs 18%; P<.001). Based on their findings, those authors suggested obesity was a consequence of psoriasis rather than a risk factor for the skin disease. In addition, a study by Neimann12 demonstrated that the risk of obesity was higher in patients with severe psoriasis (odds ratio [OR],1.8) than in those with moderate psoriasis (OR,1.3).
The idea of a connection between nutrition and the clinical course of psoriasis arose when symptomatic improvement was observed during periods of fasting or lower calorie intake.13 The Bardazzi research group,14 with a sample of 33 patients with moderate to severe psoriasis, reported a greater response to biological therapy in those patients who reduced their BMI, even with reductions of as little as 5kg body weight over 8 months of follow-up. In a study performed in Croatia involving 82 patients with a 10-year history of psoriasis vulgaris treated using standard topical treatment, 40 patients received the usual hospital diet and 42 received a low-calorie diet.15 After 4 weeks, the low-calorie-diet group showed a statistically significant improvement in their skin lesions compared to the control group. In another study involving 61 obese patients with moderate or severe psoriasis on treatment with low-dose ciclosporin, the response to the drug was considerably better in the group receiving a low-calorie diet (reduction of 500kcal/day) than in the control group with no change in calorie intake.16
Those studies coincide in proposing a low-calorie diet as coadjuvant therapy in the management of psoriasis. It would therefore be interesting to reach a better understanding of this association and to develop useful tools for the nutritional management of these patients in the dermatology clinic.
Obesity and InflammationObesity is currently considered to be a low-grade chronic inflammatory disease characterized by an elevation of the plasma levels of proinflammatory cytokines, such as tumor necrosis factor (TNF) α and interleukin (IL) 6, and of acute-phase proteins such as C-reactive protein (CRP).17 The association of psoriasis with obesity may be explained by the specific inflammatory activity of the adipocytes. Adipose tissue, typically thought of as an energy store, is able to communicate with the rest of the body through the secretion of adipokines, which are molecules with proinflammatory, thrombotic, and vasoactive properties.18
Particularly important adipokines are TNF-α, plasminogen activator inhibitor 1, IL-6, and leptin. There is also a fall in the levels of adiponectin, a cytokine with anti-inflammatory activity.19 These signals attract macrophages to the adipose tissue. After entering the adipose tissue, mature macrophages maintain the cytokine secretion, leading to a local primary inflammatory response. The cytokines subsequently trigger the production of inflammatory proteins in the liver, thus causing the low-grade systemic inflammatory state observed in obesity.20 Cytokines also increase lipolysis, leading to a constant release of free fatty acids from the adipose tissue into the peripheral circulation.19 Free fatty acids are considered to be an important link between adipose tissue activity and chronic inflammation as they can increase oxidative stress and thus augment the inflammatory environment and vascular activity.21 It should be noted that predominantly central obesity, compared with a peripheral distribution of fat, is associated with a large amount of visceral fat. Adipocytes in the visceral fat are metabolically more active and they release larger quantities of cytokines and fatty acids. This would lead us to expect an even more active inflammatory environment in patients with abdominal obesity.22
Foods have also been implicated in inflammation. Aijada et al23 showed that eating fast food (900kcal, rich in fats and simple sugars) could lead to an increase in inflammatory factors such as CRP. This effect would be mediated by the activation of the nuclear factor kappa B (NF-κB) present in the white blood cells; the transcriptional activity of NF-κB is related to the release of free oxygen radicals and cytokines with inflammatory activity. This same effect was observed after administering an intravenous infusion of triglycerides to healthy individuals.21
It has been suggested that the inflammatory state associated with obesity is the link between various pathological conditions that make up the metabolic syndrome.24 The effect of the cytokines on insulin sensitivity in the liver25 and muscle26 has been studied extensively, whereas the association between psoriasis and obesity has only been demonstrated clinically in recent decades,27,28 and there has been no detailed study of the molecular mechanisms involved. However, psoriasis and obesity are both inflammatory disorders, and the pathophysiological changes, including inflammatory pathways and elevated cytokine levels, are similar in the 2 conditions.1 From this point of view, it would appear reasonable to suggest that a reduction in energy intake, with the consequent weight loss, could contribute positively to reducing the proinflammatory state and improving the clinical course of obese patients with psoriasis.
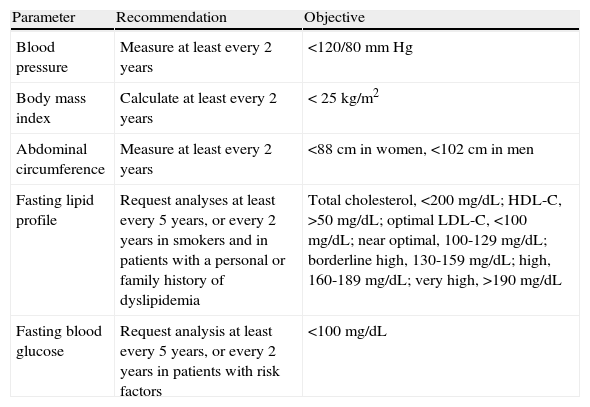
RecommendationsThe high prevalence of comorbid diseases in patients with psoriasis means that they would benefit from a holistic approach with multisystem management.29 It is particularly important to stratify patients according to their cardiovascular risk. For this purpose, the National Psoriasis Foundation30 recommends adherence to the current guidelines for screening and goals for cardiovascular risk factors established by the American Heart Association (AHA)(Table 1).31 Those guidelines have been modified with lower cutoff points for cholesterol levels in patients with high cardiovascular risk. Specialist consultation is recommended in these cases in order to avoid any delay in the initiation of aggressive management of the metabolic parameters.32
American Heart Association Proposed Recommendations for the Detection of Cardiovascular Risk Factors.
| Parameter | Recommendation | Objective |
| Blood pressure | Measure at least every 2 years | <120/80mm Hg |
| Body mass index | Calculate at least every 2 years | < 25 kg/m2 |
| Abdominal circumference | Measure at least every 2 years | <88cm in women, <102cm in men |
| Fasting lipid profile | Request analyses at least every 5 years, or every 2 years in smokers and in patients with a personal or family history of dyslipidemia | Total cholesterol, <200 mg/dL; HDL-C, >50 mg/dL; optimal LDL-C, <100 mg/dL; near optimal, 100-129 mg/dL; borderline high, 130-159 mg/dL; high, 160-189 mg/dL; very high, >190 mg/dL |
| Fasting blood glucose | Request analysis at least every 5 years, or every 2 years in patients with risk factors | <100 mg/dL |
Abbreviations: HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
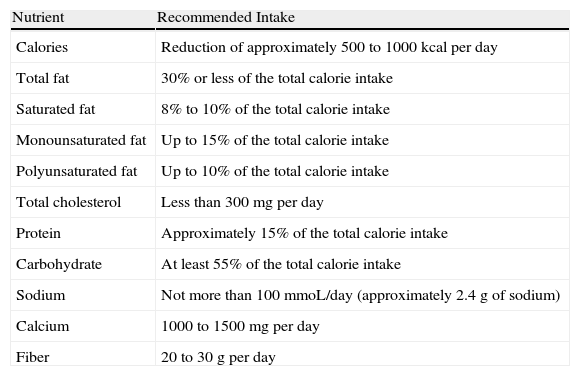
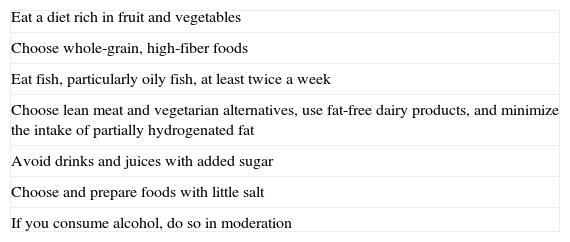
All patients, and particularly those with a BMI over 25, should be instructed in nonpharmacological measures aimed at lifestyle changes. The objective is to achieve healthy eating habits that can be maintained over time and that will result in controlled weight loss. A low-calorie diet based on the Step 1 diet (Table 2) should be recommended.33 This diet involves reducing total calorie intake by 500 to 1000kcal per day, depending on the patient's energy expenditure. An individual's energy expenditure at rest can be calculated using measurement techniques, such as indirect calorimetry, or mathematical formulae, the most widely used of which is the Harris-Benedict formula (Table 3), which takes into account parameters such as sex, age, and height.34 To achieve good adherence to the dietary therapy, we recommend application of the practical recommendations proposed by the AHA (Table 4).35 Patients with severe obesity (BMI >40) should be referred to a specialist to consider surgical treatment. The effectiveness of this type of procedure in the remission of comorbid conditions and in the long-term maintenance of body weight makes it the treatment of choice in patients with severe obesity.36 There have recently been case reports describing patients with psoriasis whose lesions have shown a marked improvement within months of undergoing gastric bypass surgery.37,38
The Low-Calorie Step I Diet.
| Nutrient | Recommended Intake |
| Calories | Reduction of approximately 500 to 1000kcal per day |
| Total fat | 30% or less of the total calorie intake |
| Saturated fat | 8% to 10% of the total calorie intake |
| Monounsaturated fat | Up to 15% of the total calorie intake |
| Polyunsaturated fat | Up to 10% of the total calorie intake |
| Total cholesterol | Less than 300mg per day |
| Protein | Approximately 15% of the total calorie intake |
| Carbohydrate | At least 55% of the total calorie intake |
| Sodium | Not more than 100 mmoL/day (approximately 2.4g of sodium) |
| Calcium | 1000 to 1500mg per day |
| Fiber | 20 to 30g per day |
American Heart Association Nutrition Committee Practical Recommendations to Keep to a Healthy Diet.
| Eat a diet rich in fruit and vegetables |
| Choose whole-grain, high-fiber foods |
| Eat fish, particularly oily fish, at least twice a week |
| Choose lean meat and vegetarian alternatives, use fat-free dairy products, and minimize the intake of partially hydrogenated fat |
| Avoid drinks and juices with added sugar |
| Choose and prepare foods with little salt |
| If you consume alcohol, do so in moderation |
Physical activity should be indicated on an individual basis according to age, tolerance, preference, etc.35 Ideally, patients should start with 30minutes of physical activity 3 times a week,30 but a metabolic effect with major benefit is obtained with at least 150minutes of moderately intense physical activity per week.39 Furthermore, patients must stop smoking, as this is known to exacerbate psoriasis.30
Specialist management is essential when comorbid psychiatric and psychological conditions are detected.40
Finally, current evidence indicates that it is essential to take all comorbid metabolic conditions into account before deciding which pharmacological therapy to prescribe for psoriasis.41 Conditions such as obesity and nonalcoholoic fatty liver or steatohepatitis are relative contraindications for the use of methotrexate, due to the risk of hepatic toxicity.42,43 Some immunomodulating biologic agents, such as alefacept, etanercept, and ustekinumab, are less effective in obese patients, whereas others, such as infliximab, whose dose must be adjusted according to the BMI, maintain their effectiveness.41 In addition, obesity, hypertension, and dyslipidemia interfere with the use of ciclosporin as they increase the risk of nephrotoxicity.41,44
DiscussionConventional psoriasis treatments are based on the severity of the disease. The need for safe and effective treatments has led to a search for modifiable factors that could improve the response to conventional therapy.45
The pathophysiology of psoriasis and of obesity have common inflammatory pathways and cytokine activation.46 Clinical studies have strengthened the idea that weight loss could have an additional therapeutic effect in the conventional treatment of obese patients with psoriasis, particularly in those with moderate to severe disease.14
Furthermore, psoriasis should be considered to be a specific cardiovascular risk factor. A higher incidence of ischemic events has been reported in these patients independently of their other cardiovascular risk factors.3,47 A possible benefit in the reduction of cardiovascular risk has also been attributed to immunomodulatory treatment with TNF-α inhibitors.48 We hope that the international guidelines for cardiovascular risk prevention will take these findings into consideration in the future.
Education regarding modifiable factors (healthy eating, maintenance of an appropriate weight, physical activity, and quitting smoking) is therefore essential in the treatment of this disease and is one of the primary interventions that can affect the prognosis of patients with psoriasis.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Farías MM, et al. Psoriasis y obesidad: revisión y recomendaciones prácticas. Actas Dermosifiliogr. 2011;102:505-9.



