




Repair of distal nasal defects resulting from Mohs micrographic surgery is a challenge, but surgeons can choose from a number of techniques. We present 3 cases in which an east-west flap was used to close the defect. The east-west flap is an easily conceived advancement flap that consists of a superior triangle used to cover the defect and an inferior triangle whose base is located along the advancement line. The flap results in an optimal cosmetic outcome and involves minimum movement of tissue (preserving the nasal architecture) and well-camouflaged suture lines.
La reparación de los defectos nasales distales producidos durante la cirugía micrográfica de Mohs representa un desafío para el cirujano. Existen múltiples técnicas por las cuales se puede optar para el cierre del defecto. Presentamos 3 casos en los que se realizó el colgajo este-oeste, un colgajo de avance, de fácil diseño, que consiste en un triángulo que cubre el defecto y un segundo triángulo de descarga con sus bases en la línea de desplazamiento. Con este colgajo se obtiene un óptimo resultado estético con un movimiento mínimo de los tejidos, preservando la arquitectura nasal y con líneas de sutura bien disimuladas.
Repair of distal nasal defects resulting from Mohs micrographic surgery is a challenge, but surgeons can choose from a number of techniques. We present 3 cases in which an east-west flap was used to close the defect. The east-west flap is an easily conceived advancement flap that consists of a superior triangle used to cover the defect and an inferior triangle whose base is located along the advancement line. The flap results in an optimal cosmetic outcome and involves minimum movement of tissue (preserving the nasal architecture) and well-camouflaged suture lines.
IntroductionSkin cancer accounts for a third of malignant tumors in humans, and nonmelanoma tumors and basal cell carcinomas account for about 80% of skin cancers. These tumors are usually located on sun-exposed skin, especially the T-zone and in patients with low-phototype skin or chronic sun damage. The face is a high-risk zone for any size lesion. Once a lesion is removed surgically, a firm diagnosis can be reached and tumor-free margins confirmed. Mohs micrographic surgery (MMS) is able to preserve as much healthy tissue as possible, and all margins can be inspected. MMS is associated with lower recurrence rates than conventional surgery and has been shown to be effective in the treatment of nonmelanoma skin cancer.1,2
The surgeon must choose the optimal approach for closing the post-MMS defect. Closure on the nose, where most nonmelanoma tumors are found,2 is challenging. Available techniques are direct closure, flaps, grafts, or second-intention healing. Skin flaps have the advantage of advancing skin from the surrounding area, and they provide a good blood supply.3,4 We describe our experience in 3 cases in which east-west flaps were used to repair defects after MMS.
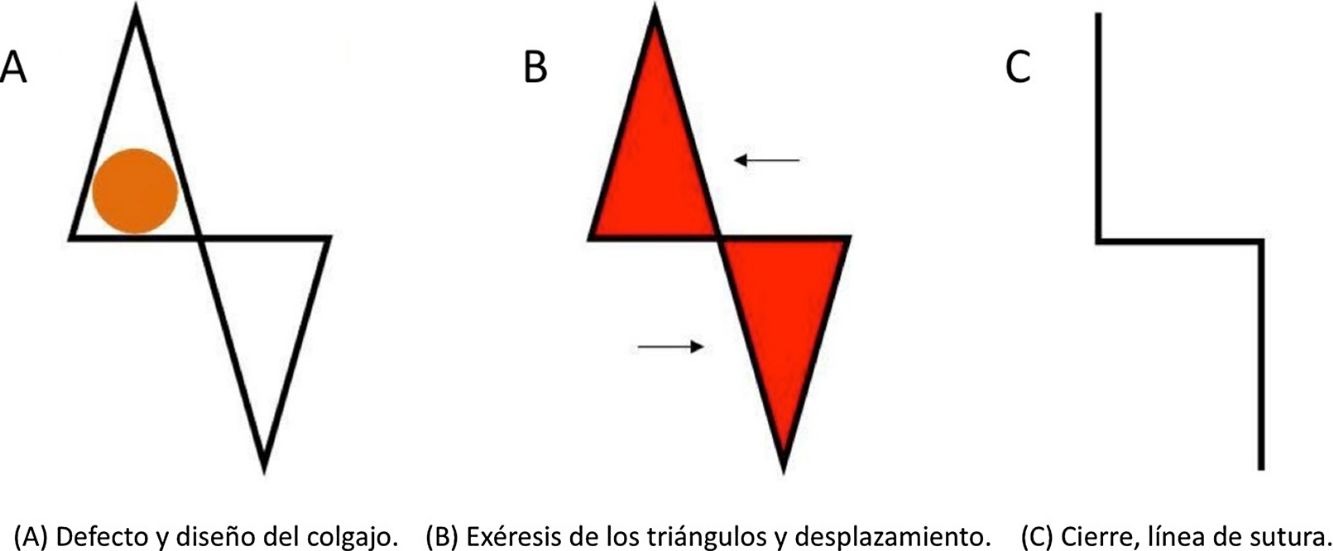
The east-west advancement flap, a technique first described by Perry Robins, is often used to repair small defects of less than 1.5cm in diameter on the nose and nearby areas.5–8 It allows skin to be advanced in a single direction and is designed by making a vertical triangle superior to the defect and another release triangle inferior to it. The base of the inferior triangle will be half the width of the primary defect and its overall size will be similar to the first triangle's.8 The height of the triangles will be the same, and a larger defect will require a larger release triangle.6,8 The flaps should be undermined below the muscle and above the perichondrium so the tissue can slide horizontally toward the defect.6 Three perpendicular sutures anchor the flaps (Fig. 1).
.")
This study aimed to describe patient and physician assessments of the cosmetic outcomes of east-west flap repairs 6 months after MMS. Two dermatologists who did not treat the patients evaluated the results based on standardized photographs taken at the 6-month follow-up visits. Outcomes were classified as excellent, very good, good, fair, poor, or very poor.
Case DescriptionsCase 1A 72-year-old man with phototype/III skin was treated for a nodular basal cell carcinoma on the nasal tip. It measured 0.4×0.5cm on the nasal tip (Fig. 2A) and had appeared 9 months earlier. The lesion was removed in a single stage of MMS, leaving a surgical defect measuring 1×0.9cm that was closed with an east-west advancement flap. There were no complications and both the dermatologists and the patient evaluated the results as good (Figs 2B and 2C).
Case 2, their results immediately after surgery (B, E, and H), and their results at the 6-mo follow-up visits (C, F, and I).")
A 42-year-old woman, a smoker with phototype-IV skin, was treated for an ulcerated nodular basal cell carcinoma measuring 0.5×0.4cm that had appeared on the nasal tip approximately 12 months earlier (Fig. 2D). The 1×1-cm defect left by 2-stage MMS was repaired with an east-west flap. There were no complications. The 2 dermatologists described the outcome as good and the patient assessed it as very good (Figs. 2E and 2F).
Case 3A 75-year-old man with phototype-III skin who had undergone several surgeries for nonmelanoma skin cancer was treated for a nodular basal cell carcinoma measuring 0.8×0.7cm on the nasal tip that had appeared 6 months earlier (Fig. 2G). It was removed by MMS in a single stage. The defect, which measured 1.2×1.2cm, was repaired with an east-west flap. There were no complications and both dermatologists and the patient evaluated the results as excellent (Figs. 2H and 2I).
At the 6-month follow-up visits there were no signs of recurrence. The patients continue to be followed in accordance with current protocols.
DiscussionMany different flap techniques have been described for repairing nasal defects after MMS. The size of the defect and the anatomical location must be considered when selecting a technique that will preserve function and provide a cosmetically satisfactory outcome.2,4 We chose the east-west flap as ideal for the characteristics shared by the patients in this series.
This flap has a number of advantages. It facilitates the repair of small defects; provides a robust vascular pedicle and good tissue compatibility; minimizes tension; and preserves nasal architecture, symmetry, texture and color.8 Both functional and cosmetic outcomes are excellent 6 months after surgery.5–7
The east-west flap is used mainly on large or long noses with defects that are longer than they are wide and located on sebaceous skin.6–8 Our patients met these criteria.
A limitation of this flap is the difficulty of using it to repair medium-sized or large defects. It is also problematic in certain nasal locations, such as at the lower sidewalls, the edges of the alae, and the narrower portion of the tip.5–8
The east-west flap is also a good choice for repairing defects on other facial structures, such as the upper lip, the eyelids, the external ear, and the cheek.9,10 These are all locations where there is extra tissue available for flaps.10
The east-west flap is simpler than the bilobed flap, although the latter is preferred for closing paramedian nasal defects and may even be superior to transposition flaps (which can lead to tissue distortion) and to rotation flaps (which require larger incisions in nonexposed areas).5–8
To conclude, these surgical defect repairs are challenging. The east-west flap is indicated for small defects of less than 1.5cm in diameter at the tip of the nose, where it provides excellent functional and cosmetic results.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Magliano J, Abelenda MP, Navarrete J, Bazzano C. Colgajo este-oeste después de la cirugía micrográfica de Mohs.Eczema y urticaria en Portugal. 2019;110:759–762.



