

Intravenous gamma globulin (IVGG) therapy is a treatment based on blood products obtained from multiple donations. It has been used for decades to treat a variety of skin diseases, including autoimmune blistering diseases, some forms of collagenosis, and severe toxic drug reactions.1,2
Our patient was a 60-year-old woman who had undergone surgery for ovarian adenocarcinoma and had rheumatoid arthritis, for which she was in treatment with sulfasalazine and leflunomide. She came to the emergency department with a cutaneous presentation that had appeared 72 hours earlier and consisted of oral discomfort and conjunctivitis, followed by the appearance of target lesions in the cervical area and on both palms and soles. In some areas, including the labial submucosa, the lesions caused erosions, and tense blisters were observed on the acral surface. The patient occasionally took paracetamol or tramadol, had completed a cycle of amoxicillin/clavulanic acid (875/125 mg for 2 months), and during the preceding 2 weeks had been using Perio-Aid rinses (0.12% chlorhexidine, 0.05% cetylpyridinium chloride) prescribed by her dentist. She had been exposed once to Artinibsa (articaine + epinephrine, 40 mg/mL), which was used as an anesthetic for a tooth extraction procedure. Serology for Mycoplasma species was negative. Based on a suspected diagnosis of Stevens-Johnson syndrome, the patient was hospitalized in the dermatology ward for systemic treatment with prednisone (1 mg/kg/d). On the second day after admission, the rash on the trunk, neck, and face became more pronounced, and multiple erosive areas appeared, for which she began IVGG treatment (Plangamma®, 0.4 g/kg/d) for 5 days. However, on the day of completion of IVGG treatment, the rash continued to progress and the erosive areas already exceeded 20–30% of the body surface. Blood was extracted for baseline blood tests and a single dose of etanercept (50 mg) was prescribed and administered without waiting for the blood test results. Over the next 48 hours, the patient’s general condition progressively improved, and there was an evident interruption of the progression of her condition. The serological findings indicated possible past hepatitis B virus (HBV) infection (positive for hepatitis B core antibody [HBcAb] IgG and hepatitis B surface antibody [HBsAb]) that had not been detected in blood tests performed 7 months earlier. The patient was negative for hepatitis B surface antigen (HBsAg) and for hepatitis B viral DNA, as evaluated by polymerase chain reaction. The patient’s clinical history revealed no risk factors for HBV. Therefore, possible passive acquisition of HBcAb and HBsAb through IVGG therapy was suspected. This suspicion was confirmed 6 weeks later when the patient tested negative for HBcAb.
Evaluation of HBsAg and viral DNA is mandatory for screening of HBV to prevent virus transmission in blood products. However, this analysis does not exclude donors with past HBV infections, who can transmit their protective antibodies to IVGG recipients.3 In fact, in a cohort of 80 patients treated with IVGG in which 9 patients were HBsAb-positive and 1 patient was a doubtful positive for HBcAb before receiving infusions, the percentage of patients positive for HBsAb and HBcAb IgG increased to 99% and 46%, respectively, after treatment.4 A lack of knowledge of this condition can result in the incorrect diagnosis of IVGG recipients with latent infections, leading to stress and unnecessary treatment5 (e.g. in patients who will subsequently be treated with rituximab for autoimmune blistering diseases).6,7 Another infection that can cause confusion is syphilis, since IVGG infusions can contain antibodies that are identified in treponemal tests, although reagin tests are always negative.5,8 Cases have been described in which patients treated with IVGG have tested positive forToxoplasma9 and Borrelia burgdoferi10 (Table 1). Positivity for pathogens against which the population is frequently immunized, including varicella-zoster virus and parvovirus B19, can also be expected after IVGG therapy.
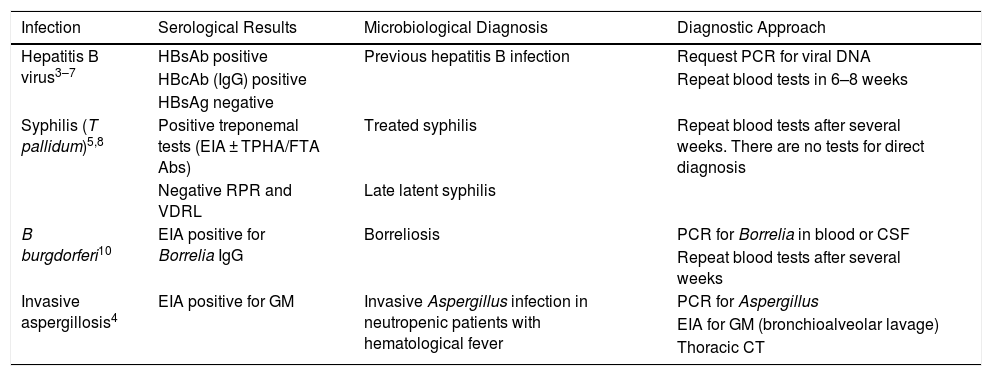
Positive Serological Results Reported in Intravenous Gamma Globulin Recipients, Microbiological Diagnosis That Patients Would Have Received if not Exposed to Gamma Globulins, and Approach Taken to Verify a False-positive Caused by Passive Antibody Transfusion
| Infection | Serological Results | Microbiological Diagnosis | Diagnostic Approach |
|---|---|---|---|
| Hepatitis B virus3–7 | HBsAb positive | Previous hepatitis B infection | Request PCR for viral DNA |
| HBcAb (IgG) positive | Repeat blood tests in 6–8 weeks | ||
| HBsAg negative | |||
| Syphilis (T pallidum)5,8 | Positive treponemal tests (EIA ± TPHA/FTA Abs) | Treated syphilis | Repeat blood tests after several weeks. There are no tests for direct diagnosis |
| Negative RPR and VDRL | Late latent syphilis | ||
| B burgdorferi10 | EIA positive for Borrelia IgG | Borreliosis | PCR for Borrelia in blood or CSF |
| Repeat blood tests after several weeks | |||
| Invasive aspergillosis4 | EIA positive for GM | Invasive Aspergillus infection in neutropenic patients with hematological fever | PCR for Aspergillus |
| EIA for GM (bronchioalveolar lavage) | |||
| Thoracic CT |
Abbreviations: Ab, antibody; Ag, antigen; CT, computed tomography; CSF, cerebrospinal fluid; EIA, enzyme immunoassay; FTA Abs, fluorescent treponemal antibody absorption test; GM, galactomannan; HBcAb, hepatitis B core antibody; HBsAb, hepatitis B surface antibody; IgG, immunoglobulin G; IVGG, human intravenous gamma globulin; PCR, polymerase chain reaction; RPR, fast plasma reagin; TPHA, Treponema pallidum hemagglutination assay; VDRL, Venereal Disease Research Laboratory test.
Therefore, in patients treated with IVGG, positive microbiological serology results should be interpreted with caution. For some pathogens, such as T pallidum, B burgdorferi, and Toxoplasma, serology should be repeated 4 to 8 weeks later (the half-life of IgG is 3 weeks) and again until values return to normal. If available, molecular diagnostic techniques (e.g. HBV DNA detection) should be requested, as these can more quickly rule out an active infection.
Furthermore, if IVGG is used to treat diseases that may subsequently require the use of biological drugs such as rituximab, it may be advisable to have baseline serology data at hand, as this will facilitate interpretation of the results of pretreatment screening studies after IVGG infusion.
The authors thank the allergology service, and especially Pilar Tornero for her tireless work with patients with allergic skin reactions. Thanks also to the hospital’s intensive care service for their assistance in the management of this case.
Please cite this article as: Sánchez-Herrero A, Nieto-Benito LM, Rosell-Díaz AM, Pulido-Pérez A. Falsa positividad serológica para la hepatitis B tras el empleo de inmunoglobulinas intravenosas para una necrólisis epidérmica tóxica. Actas Dermosifiliogr. 2021;112:476–477.



