

Japan has suffered one of the worst earthquakes in the history of humanity (9 points on the Richter scale) followed by a devastating tsunami with waves over 20 meters high, and the country is now facing the consequences of the serious damage to some of its nuclear power plants, in particular Fukushima. The accident has sparked fear worldwide concerning the potential risks of nuclear radiation. I believe that it is of interest to explain some important concepts regarding radioactivity,1 the real risks to human health and, as we are dermatologists, the cutaneous manifestations observed in cases of exposure to ionizing radiation.
The core of a nuclear reactor contains over 60 radioactive contaminants, the products of uranium fission. The radioactive particles released in the course of the Fukushima nuclear emergency were mostly iodine 131 and cesium 137; radioactive iodine, which has a half-life of 8 days, is taken up by the thyroid gland, and cesium, with a half-life of 30 years, is deposited in the muscles. Plutonium leaks were also detected. In the Chernobyl accident, by contrast, due to the explosion of one of the nuclear reactors, large amounts of strontium 90 and some of the nuclear fuel (uranium) and its decay product (plutonium) were also released. These reaction products are much more dangerous to health and have a much longer half-life.1
Radioactive substances emit ionizing radiation, that is, radiation that has enough energy to ionize matter by removing electrons that are bound to an atom. This process produces free radicals, which directly damage DNA and cell proteins and result in radiation-induced genomic instability.2 Non-ionizing radiation (electromagnetic fields and electromagnetic radiation in the visible spectrum) does not have this effect.
Ionizing radiation also occurs at low levels in nature, and there are various types, as follows:
- •
Alpha particles (2 protons and 2 neutrons)
- •
Beta particles (an electron or a positron)
- •
Gamma rays (photons)
- •
X-rays
- •
Neutrons
The dose of ionizing radiation absorbed by matter is measured in grays (Gy). The effective dose absorbed by an organism is measured in sievert (Sv), a unit that takes into account both the type of ionizing radiation and the biological effects produced. In Spain, we are exposed to a dose of between 2.4 and 3 millisieverts (mSv) per year. (In Fukushima, levels thousands of times greater than the permitted threshold have been detected.) Exposure to an annual dose below 100 mSv is considered to be safe.1
Some of the effects of ionizing radiation are stochastic or random rather than dose dependent and may occur after low-level exposure, although the probability of damage increases with the dose received. There are also dose-dependent deterministic effects. The physical repercussions of ionizing radiation depend on the individual's distance from the radiation source, the sensitivity of each type of tissue, the absorbed dose rate, and the radioactive materials involved.1 Ionizing radiation has been classified as a confirmed carcinogen by the International Agency for Research on Cancer. It can cause every type of cancer except mesothelioma.2,3
Exposure to a megadose, as in the case of a nuclear accident, can cause acute radiation syndrome (a 5000 mSv single dose would kill approximately half of the exposed population within 1 month).3–7 In such circumstances, four phases would be observed8:
- 1.
The prodromal phase: anorexia, apathy, nausea, vomiting, diarrhea, fever, tachycardia, and headache, occurring between 2 and 6 days after exposure.3
- 2.
The latent phase: transient improvement lasting between several days and 1 month. The duration of the latent phase is inversely related to the dose received.
- 3.
Manifest disease phase: intense immunosuppression and pancytopenia that may result in complete myelosuppression. Central nervous system involvement giving rise to headache, cognitive deficits, hyporeflexia, and stroke Gastrointestinal symptoms: diarrhea, abdominal pain, and gastrointestinal bleeding. Skin disease, which will be discussed below. Treatment requires individualized life support measures (fluids, antibiotics, platelets, granulopoietic cytokines, transfusions, hematopoietic cell transplantation), and the administration of potassium iodide at doses of 130mg/d in adults.3,4,7
- 4.
Death or recovery phase: survivors will require lifelong follow-up due to the long-term risk of carcinogenesis and to treat sequelae
Cutaneous radiation syndrome or radiation dermatitis is also seen following iatrogenic exposure.3–8 There are acute and chronic clinical manifestations. Acute radiation dermatitis is caused by high-energy radiation and develops after a latent period of 6 to 12 days following exposure and with cumulative doses of more than 7Gy. Depending on severity, radiation dermatitis is classified as:
- 1.
First degree: erythema that resolves leaving diffuse or mottled hyperpigmentation. Exposure of 3Gy or more produces transient alopecia and reduced sebaceous gland activity. These manifestations develop some 3 weeks after exposure and resolve between 4 and 12 weeks.
- 2.
Second degree: this develops after exposure to doses ranging from 8 to 10Gy and takes the form of erythema, edema, and blistering. It is also associated with permanent loss of hair, sebaceous glands, sweat glands, and nails.
- 3.
Third degree: deep necrosis, slow-healing scabs and ulcers associated with sequelae, and an increased risk of squamous cell carcinoma.
Chronic radiation dermatitis occurs with doses above 12 to 15Gy and develops after a latency period of 2 years. The clinical features include atrophic and sclerotic skin, loss of appendages, hyper- or hypopigmentation, and telangiectasia. The risk of ulcers and skin cancer is high (these form on precursor lesions called roentgen keratoses, which are similar to actinic keratoses).
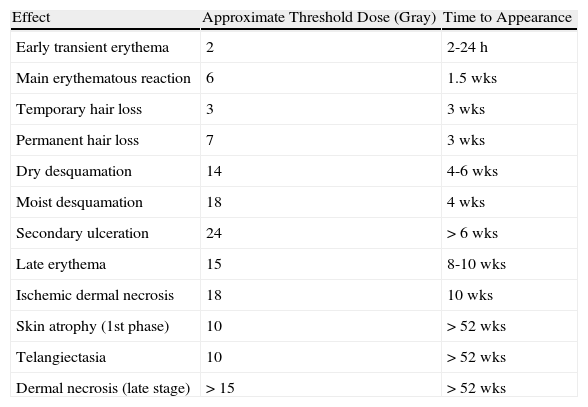
In both acute and chronic disease, involvement tends to be patchy since non-irradiated basal cells give rise to clones that generate patches of healthy skin, which are surrounded by diseased areas. Table 1 summarizes the main reactions of human skin to ionizing radiation and the threshold dose and time to occurrence of each reaction.5
Principal Effects of Ionizing Radiation on the Skin: Threshold Dose and Time to Appearance.5
| Effect | Approximate Threshold Dose (Gray) | Time to Appearance |
| Early transient erythema | 2 | 2-24 h |
| Main erythematous reaction | 6 | 1.5 wks |
| Temporary hair loss | 3 | 3 wks |
| Permanent hair loss | 7 | 3 wks |
| Dry desquamation | 14 | 4-6 wks |
| Moist desquamation | 18 | 4 wks |
| Secondary ulceration | 24 | > 6 wks |
| Late erythema | 15 | 8-10 wks |
| Ischemic dermal necrosis | 18 | 10 wks |
| Skin atrophy (1st phase) | 10 | > 52 wks |
| Telangiectasia | 10 | > 52 wks |
| Dermal necrosis (late stage) | > 15 | > 52 wks |
The treatment of acute radiation dermatitis is symptomatic and involves the application of emollients and topical corticosteroids. Indometacin and other nonsteroidal oral anti-inflammatory drugs may help to reduce pain and edema. Granulation tissue does not form in chronic radiation dermatitis, and treatment is limited to surgical debridement and skin grafting. Carcinomas and roentgen keratoses are treated in the conventional manner.7
DedicationTo all of those working every day to control the radiation leaks in Fukushima, Japan.
When a leak is detected in a radioactive installation, measures must be taken to prevent contamination, such as those that were implemented following the Fukushima accident:
- 1.
Contact with the skin can be eliminated by thorough washing with detergent and disposal of clothes.
- 2.
Iodine is the only effective measure in the case of particle inhalation. The iodine saturates the thyroid gland, thereby preventing the uptake of radioactive iodine. However, this measure provides no protection against cesium or strontium uptake.
- 3.
A total exclusion zone with a radius of 20 to 30 kilometers around the source of radioactivity (irrespective of political boundaries) in which no civilians are permitted to remain is complemented by a second peripheral area in which people remain ready for evacuation and must stay inside their homes with the doors and windows tightly closed. The IAEA (International Atomic Energy Agency) monitors radiation levels at various distances from the source and orders the appropriate preventive measures.
- 4.
The nuclear fallout is deposited on the land and in the sea, where it is incorporated into the trophic chain, contaminating plants and animals. To reduce the risks the authorities may place a temporary ban on the sale of products originating in the affected area. Other countries may also impose bans or restrictions on imports from the affected areas. In any case, rigorous monitoring of radioactivity levels in agricultural and food products is essential.
Please cite this article as: Fueyo-Casado A, Pedraz-Muñoz J. Fukusima: lo que el dermatólogo debe saber. Actas Dermosifiliogr.2011;102:631-644.



