


Although nail dermoscopy was initially used only to assess nail pigmentation, it is now widely used to study many nail disorders.
In our routine clinical practice, dermoscopy may confirm clinical diagnoses and guide the management of nail diseases and treatments.
This is the case of giant subungual wart in a 6-year-old girl with which we can discuss the value of dermoscopy regarding positive and differential diagnoses.
A 6-year-old girl presented with a 6-month history of a large subungual tumor on her right thumb nail. Examination revealed brown subungual hyperkeratosis and onycholysis (Fig. 1).

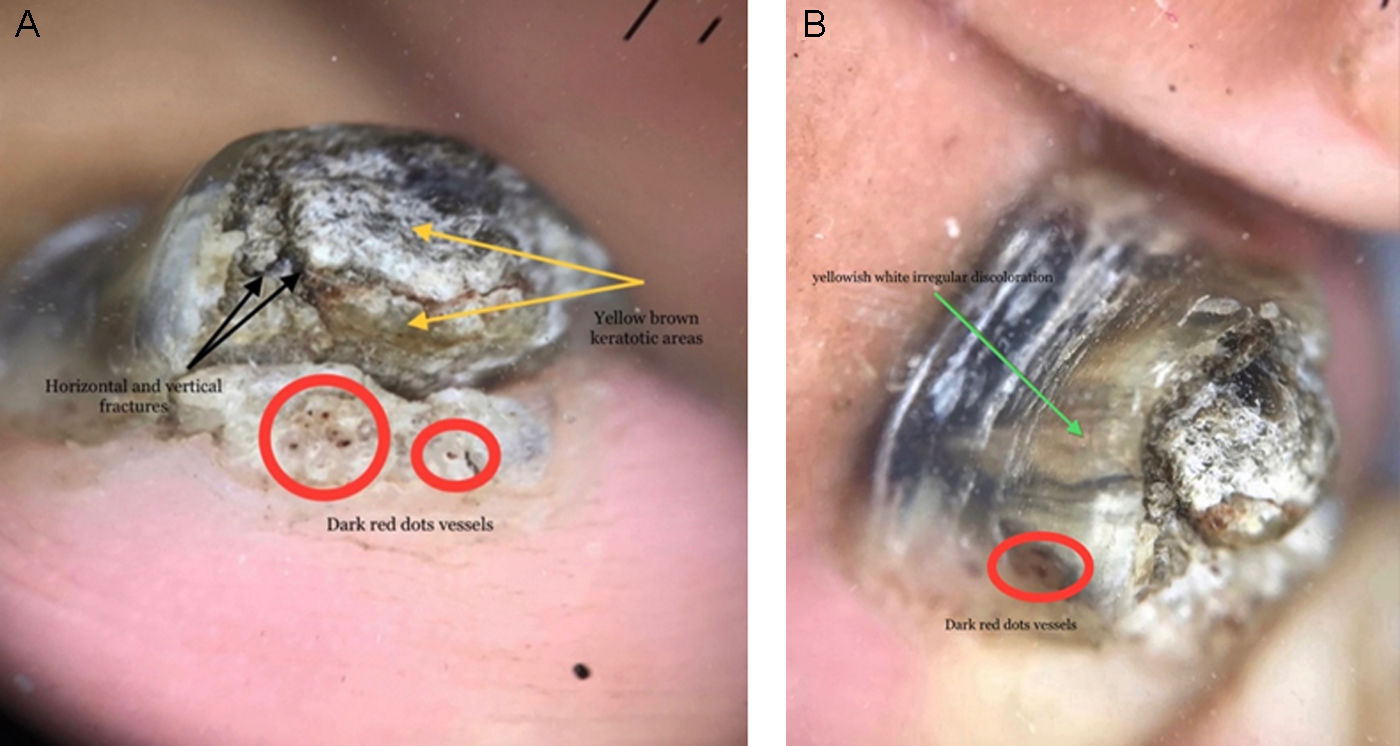
Dermoscopy of the nail free edge revealed yellowish brown keratotic areas with white scales, horizontal and vertical fractures arranged in a frogspawn pattern (Fig. 2A), while onychoscopy of the nail plate revealed yellowish white irregular discoloration (Fig. 2B). Post-excision histopathology confirmed the diagnosis of wart.
 Dermoscopy of the nail free edge: yellowish brown keratotic areas with scales (yellow arrow) and horizontal and vertical fractures (black arrow) arranged in a frogspawn pattern (red circle). (B) Dermoscopy of nail plate: yellowish white irregular discoloration (green arrow).")
Warts are common infections in children and adolescents due to the human papilloma virus. Subungual localization is a common finding, recurrent particularly in children, and usually painful. The giant subungual form is rare and may be confused with onychomycosis and other subungual tumors such as Bowen disease, subungual exostosis, squamous cell carcinoma, and onychomatricoma.
The advantage offered by dermoscopy is that it guides positive diagnosis. For giant subungual warts, dermoscopy of the free edge and hyponichium shows thick, adherent, white-yellow scales, fissures, and dilated dotted vessels surrounded by a white halo. Yellowish white irregular discoloration of the tablet along with hemorrhagic vessels are often observed when examining the nail plate.1
Bowen disease of the nail fold is one of the main differential diagnoses of subungual warts. Advanced age, recurrent and recalcitrant nature are elements that often signal Bowen's disease. Dermoscopy can also be helpful and suggest the diagnosis of Bowen's disease by revealing a yellowish verrucous surface, brown-red streaky hemorrhages – and focally – glomerular vessels with white perivascular halos.2
Subungual exostosis – the most common nail tumor in young adults – is a benign bony proliferation of the distal phalanx that occurs underneath the nail, whose diagnosis is essentially radiological, yet dermoscopy can guide the diagnosis. The main dermoscopic signs of this bone tumor are vascular ectasia, hyperkeratosis, onycholysis, ulceration and circular yellow spot on the nail plate.3
Squamous cell carcinoma of the nail bed clinically presents with a subungual ulcerated nodule associated with nail plate dystrophy. Here dermoscopy shows an eroded mass, irregularly dilated vessels with several different patterns and pigmented structures included dotted purpura, grey granulation and splinter hemorrhages.4
Regarding onychomatricoma, dermoscopic examination of the plate nail shows longitudinal parallel white and grey lines on the nail tablet, splinter hemorrhages and sharply demarcated lesion edges, while the examination of the free edge of the nail plate shows honeycomb-like or Woodworm-like cavities above the curvature and thickening of the free edge.5,6
Dermoscopy of the nail tablet in onychomycosis reveals numerous signs such as a spiked and jacked pattern, longitudinal striae, aurora borealis and nail discolorations. Other features include ruin appearance, subungual hyperkeratosis, onycholysis, and distal irregular termination on the examination of hyponychium.7,8
The giant form of the subungual wart is a rare form whose clinical appearance is worrying and can mimic subungual tumors. Dermoscopy can guide the positive diagnosis which remains essentially histological.
Conflict of interestsThe authors state that they have no conflict of interests.



