





The complexity of hidradenitis suppurativa (HS) treatment calls for a multidisciplinary approach. We therefore created a multidisciplinary team to manage surgical care. This study aimed to describe the clinical characteristics of the patients we evaluated and the outcomes of the surgical techniques used.
Material and methodsDescriptive cross-sectional study of 104 patients evaluated by our surgical case management team between September 2015 and July 2018.
ResultsSurgery was used to treat 46% of the patients with HS who were evaluated. Most were men (73%) with no family history of HS (63%) and smokers or former smokers (76%). Gluteal HS comprised the largest phenotype group (41%) and the majority of cases were serious (Hurley stage II, 36%; stage III, 46%). The anatomical regions with the largest number of lesions were the axillae (51.9%) and the groin (41.3%). Surgery was most often performed in the axilla (38.3%), followed by the gluteus (23.4%). The most common drug treatment was a combination of rifampicin and clindamycin, Deroofing was the technique used most often (in 48% of the patients who underwent surgery). Postoperative outcomes were assessed as satisfactory overall in 63.4% of the cases. The HS lesion recurred in 20% and 12% developed wound dehiscence.
ConclusionsOur experience leads us to recommend forming multidisciplinary teams to improve communication between specialists, provide tailored treatment for the patient with HS, and improve follow-up.
La complejidad del tratamiento de la hidradenitis supurativa (HS) hace necesario un abordaje multidisciplinar, y con este fin diseñamos un comité quirúrgico para su abordaje. Este estudio describe las características clínicas de los pacientes evaluados y los resultados de las técnicas quirúrgicas realizadas.
Material y métodosPresentamos un estudio descriptivo transversal que recoge 104 pacientes que fueron evaluados en nuestro comité desde setiembre de 2015 hasta julio de 2018.
ResultadosEn nuestra serie, el 46% de los pacientes con HS evaluados recibieron tratamiento quirúrgico. La mayoría fueron varones (73%), sin antecedentes familiares de HS (63%), exfumadores o fumadores (76%). El fenotipo clínico predominante fue el tipo III (41%), con presencia de patología grave en la mayor parte de los casos (36% con Hurley II y 46% con Hurley III). Las áreas anatómicas más afectadas fueron las axilas (51,9%) y las ingles (41,3%); mientras que las intervenidas con mayor frecuencia fueron la axilar (38,3%), seguida de la glútea (23,4%). Entre los tratamientos médicos, el más usado fue la combinación de rifampicina con clindamicina. El destechamiento (deroofing) se posicionó como la técnica quirúrgica más empleada entre los pacientes intervenidos (hasta en un 48%). En cuanto al resultado posquirúrgico global: un 63,4% obtuvo un resultado satisfactorio, un 20% recidivó y un 12% presentó dehiscencia de la herida quirúrgica.
ConclusionesDada nuestra experiencia, recomendamos la instauración de comités multidisciplinares para mejorar la comunicación entre los diferentes especialistas, así como individualizar el tratamiento y mejorar el seguimiento de los pacientes con HS.
Hidradenitis suppurativa (HS) is a chronic disease that presents with recurrent acute inflammatory lesions in the form of nodules, fistulas, and very painful abscesses that cause poor quality of life. For this reason, HS patients often make initial contact with the health system via emergency and primary care services. It is also common for affected patients to have undergone multiple surgical interventions by different specialists, without achieving good disease monitoring or control.
Traditionally, treatment of HS has posed significant challenges, as it requires a combination of medical and surgical approaches.1 In our opinion, and in agreement with most medical centers and therapeutic guidelines, the dermatologist should propose an integrated medical-surgical approach to optimize the treatment and follow-up of HS patients, always with the assistance of the other healthcare personnel involved (colorectal surgeons, plastic surgeons, urologists, and nursing, primary care, and emergency care personnel).
The specialized HS consultation service at the Parc Taulí University Hospital in Sabadell, Spain, follows over 500 HS patients. In 2015, a multidisciplinary case management team was formed to establish consensus on the surgical treatment of HS in order to improve interactions between different specialists and optimize the treatment of our HS patients, particularly those with moderate and severe disease. The team, which meets on a monthly basis, consists of representatives from general and digestive surgery, plastic surgery, and dermatology.
The objective of the present study was to describe the characteristics and postoperative outcomes of the HS patient population evaluated by the team.
Materials and MethodsThis cross-sectional descriptive study included 104 patients who were evaluated by our multidisciplinary team between the date of its creation (September 2015) and July 2018.
The following variables were collected: clinical characteristics of the patients (sex, family history, smoking status, clinical phenotype, and disease presentation); affected and treated anatomical areas; prescribed medical treatments; surgical techniques used; and surgical outcomes.
To evaluate surgical outcomes, patients were followed up 2, 4, and 8 weeks post-surgery. A satisfactory outcome was defined as an acceptable medical and aesthetic result achieved after 3 follow-up visits, with no recurrence or surgical wound dehiscence; recurrence was defined as the presence of new HS lesions in the operated area; and surgical wound dehiscence was defined as separation of the surgical wound observed at any of the 3 post-surgical follow-up visits.
Descriptive statistics were performed for all variables, which were expressed as either absolute values or relative frequencies.
ResultsOf the HS cases reviewed by the team, 46% received surgical treatment. Patients who underwent surgery did so in general surgery (41.7%), plastic surgery (47.9%), or dermatology (10.4%). Of the patients for whom surgery was proposed, 18% did not undergo any intervention due to loss to follow-up. The remaining patients were not considered appropriate candidates for surgery at the time, and continued medical treatment while awaiting subsequent evaluation (Fig. 1).

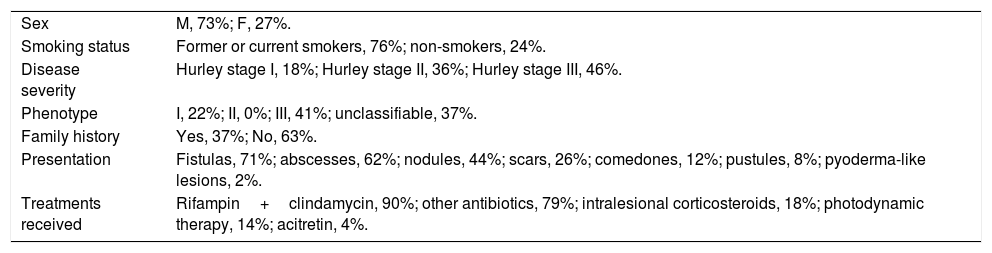
Analysis of patient characteristics revealed that the majority were men (73%), ex-smokers or smokers (76%), and had no family history of HS (63%). The predominant clinical phenotype was type III (41%), and most patients had severe pathology (Hurley stage II, 36%; Hurley stage III, 46%). Two of our patients were diagnosed with associated syndromes: one with PAPASH (pyogenic arthritis, pyoderma gangrenosum, acne, and hidradenitis suppurativa) syndrome and another with Dowling-Degos disease. The most commonly observed presentations were fistulas (71%), abscesses (62%), nodules (44%), scars (26%), comedones (12%), pustules (8%), and pyoderma-like lesions (2%) (Table 1). The most frequently affected anatomical areas were the armpits (51.9%), groin (41.3%), perianal region (36.5%), and gluteal region (26.9%). The most common sites of surgical intervention were the armpits (38.3%), followed by the gluteal region (23.4%) (Fig. 2).
Clinical Characteristics of Hidradenitis Suppurativa Cases Evaluated by the Multidisciplinary Team.
| Sex | M, 73%; F, 27%. |
| Smoking status | Former or current smokers, 76%; non-smokers, 24%. |
| Disease severity | Hurley stage I, 18%; Hurley stage II, 36%; Hurley stage III, 46%. |
| Phenotype | I, 22%; II, 0%; III, 41%; unclassifiable, 37%. |
| Family history | Yes, 37%; No, 63%. |
| Presentation | Fistulas, 71%; abscesses, 62%; nodules, 44%; scars, 26%; comedones, 12%; pustules, 8%; pyoderma-like lesions, 2%. |
| Treatments received | Rifampin+clindamycin, 90%; other antibiotics, 79%; intralesional corticosteroids, 18%; photodynamic therapy, 14%; acitretin, 4%. |
Abbreviations: F, female; M, male.

Of the medical treatments prescribed to HS patients, by far the most common was the combination of rifampicin and clindamycin at recommended doses (rifampicin [300mg/12h] and clindamycin [300mg/12h] administered orally for 10 weeks). Up to 90% of patients received this drug combination at some point during follow-up. Less frequently used treatments included other antibiotics (79%), intralesional corticosteroids (18%), photodynamic therapy (14%), and acitretin (4%) (Table 1). Finally, 18% of patients were being treated with biologic agents prior to surgery and maintained this treatment after surgery. The most commonly prescribed biologic agent was adalimumab (88%), followed by infliximab (6%) and ustekinumab (6%).
The surgical technique known as deroofing consists of lifting the roof of the fistula, cleaning the gelatinous mass from the floor of the fistula while preserving the epithelium at the base, and allowing the fistula to close by second intention. In our series, this was the most commonly used surgical technique in operated patients (up to 48%), followed by wide excision with direct closure (33.3%) and wide excision with graft or flap reconstruction (10.4%). Due to poor clinical course, 1 patient underwent a discharge colostomy and another underwent Miles amputation in general coloproctological surgery (Fig. 3).

The overall outcomes were as follows: satisfactory, 63.4%; recurrence, 20%; surgical wound dehiscence, 12%. Figure 4 shows the results obtained according to the surgical technique performed.
Discussion
While systemic agents are useful to decrease the inflammatory component of HS lesions, surgical treatment is necessary to remove the unstructured tissue that forms as a consequence of disease progression.2,3 Control of inflammation prior to surgery is currently recommended in patients with active disease. The complexity of HS management requires a multidisciplinary approach involving different specialists.
The model used to create a multidisciplinary team must be adapted to the characteristics of each center. Because some surgeries are complex and may involve wide excisions with grafts, flaps, and even colostomies or perineal amputations, other surgeons with expertise in these techniques and anatomical locations will need to provide assistance. Next, the different routes of action must be established according to the affected anatomical area, although the most appropriate route for each patient should be decided upon on a case by case basis. In general, axillary involvement was addressed in plastic surgery and perineal or gluteal involvement in general surgery. Deroofing and simple excisions were performed in dermatology.
The surgical case management team was created primarily to support the management of patients with moderate-to-severe disease who do not respond to medical treatment. For this reason, as in other surgical series,4 the percentage of patients with Hurley stages II and III was high (82%). Analysis of clinical characteristics revealed that a large proportion of patients were smokers (76%), in agreement with the findings of other case-control studies, in which the percentage of smokers was even higher in some cases (88.9%).5 The most frequently affected anatomic locations were the axillae (51.9%), the inguinal region (41.3%), and the perianal region (36.5%). In contrast to our findings, Blok et al4 reported more frequent involvement of the inguinal region than other anatomical areas (inguinal region, 85.8%; axillary region, 62.8%; and perianal region, 50.4%). In our series the most frequent sites of intervention were the axillary (38.3%) and gluteal (23.4%) regions, in line with the findings of Blok et al (22.9% and 19.8%, respectively).4
The majority of patients had been previously treated with antibiotics or other medical therapies, in accordance with the recommendations of the latest European guidelines5 for the management of HS. In our center, the most widely used surgical technique was deroofing, a simple technique that provides good medical and aesthetic results.6,7 In a prospective study by van der Zee et al8 88 HS patients underwent deroofing, with a recurrence rate of 17% after 34 months of follow-up. In our series good results were also obtained with wide excisions. While several patients who underwent this technique experienced recurrences or surgical wound dehiscence, this effect was not statistically significant owing to the limited number of patients. Other studies evaluating the rate of recurrence in patients who undergo wide excision have reported lower recurrence rates than described for other surgical techniques such as local excision or deroofing,9,10 and high rates of surgical satisfaction (up to 80%).11
In conclusion, European and Spanish guidelines for the management of HS offer recommendations but lack a clear algorithm for the surgical approach. This is mainly explained by two factors. First, there is a scarcity of data on surgical outcomes in operated HS patients. Second, classification of HS patients is hampered by the marked variability in the corresponding phenotype, and in disease severity, the locations affected, clinical course, treatment response, the degree of functional limitation, the psychological impact on the patient, and the surgeon's familiarity with surgical techniques.
This descriptive study describes the outcomes obtained in HS cases evaluated by our hospital surgical case management team. Based on our experience, we believe that multidisciplinary teams are useful to individualize treatment and improve follow-up in patients with HS, especially in cases with severe involvement or difficult-to-control disease that require combined medical and surgical treatment. We recommend the establishment of such teams in centers of reference devoted to HS. Moreover, to expand the available evidence, we believe it is necessary to conduct prospective studies comparing different surgical techniques according to the affected anatomical location.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Garbayo-Salmons P, Romaní J, Ferrer de la Fuente C, Pallisera Lloveras A, López-LLunell C, Prat Escayola J. Comité quirúrgico para la hidradenitis supurativa: nuestra experiencia. Actas Dermosifiliogr. 2020;111:408–412.



