
Dermatological complaints have been estimated to represent up to 5–10% of all the visits to emergency departments. The main objective of our study was to determine how affected is the Health related Quality of Life (HRQL) in a series of patients attending an emergency department due to skin symptoms.
Patients and methodsA prospective study during one month (July 2016) was conducted in a hospital with full-time on-call dermatologists. The Short-Form SF-12v2 Health Survey and the Dermatology Life Quality Index (DLQI) were offered to all the patients over 18 years old attending the emergency department with cutaneous complaints. Clinical and epidemiological characteristics were also collected.
ResultsIn total 108 patients completed the study. Mean age found was 45.1±16.1 years. Mean DLQI score found was 10.56±6.12. Fifty-three patients (49%) had a score of 11 or higher in the DLQI questionnaire. Most affected subscales were “Symptoms and Feelings” in DLQI scale and “Overall Health” and “Vitality” for the SF-12. A very significant difference (p<0.0001) was found between women's (12.4±5.7) and men's (7.5±5.6) DLQI mean score (mean difference of 4.9; 95% confidence interval of the difference: 2.7–7.1).
ConclusionsPatients visiting emergency units with cutaneous complaints seem to feel a moderate-large impact on their quality of life which is mainly related to the symptoms and feelings that they are experiencing. This impact is significantly higher among women.
Los problemas dermatólogicos suponen hasta un 5-10% de todas las visitas a los servicios de urgencias. El principal objetivo de nuestro estudio fue determinar la calidad de vida relacionada con la salud en una serie amplia de pacientes que acudieron a un servicio de urgencias por sintomatología cutánea.
Pacientes y métodosSe realizó un estudio prospectivo de un mes de duración (julio de 2016) en un hospital terciario con dermatólogo de guardia a tiempo completo. La versión corta del Cuestionario de Salud SF-12v2 y del cuestionario DLQI fueron entregados a todos los pacientes mayores de edad que acudieron al servicio de urgencias con problemas dermatológicos. Se recogió información clínica y epidemiológica de todos los pacientes.
ResultadosEn total, 108 pacientes completaron el estudio. La edad media de nuestra muestra fue de 45,1±16,1 años. La puntuación media del DLQI fue 10,56±6,12. Del total, 33 pacientes (49%) tuvieron una puntuación de 11 o más en el DLQI. Las subescalas más afectadas fueron la de «síntomas y sentimientos» para el DLQI y las de «salud general» y «vitalidad» para el SF-12. Se encontró una diferencia muy significativa (p<0,0001) entre las puntuaciones totales del DLQI en mujeres (12,4±5,7) y hombres (7,5±5,6), con una diferencia media de 4,9 (intervalo de confianza al 95%: 2,7-7,1).
ConclusionesLos pacientes que acuden a los servicios de urgencias con problemas dermatológicos parecen tener una afectación moderada-grave en su calidad de vida, debido principalmente a los síntomas que están experimentando. Este impacto es significativamente mayor en las mujeres.
Dermatological complaints have been estimated to represent up to 5–10% of all the visits to emergency departments.1 However, the exact incidence is very heterogeneous due to the differences that can be found amongst the methodology of previous studies in the literature regarding their duration, type of patients included or setting (hospital in-patient settings, ambulant settings or emergency departments).1–5
Cutaneous diseases might not represent a real threat to patient's life in most cases, but they are frequently felt as very disturbing due to their symptoms, such as itching or pain, or due to the fact that cutaneous lesions are easily observed by the patients. The patient's subjective sensation of alarm is what make them visit emergency departments seeking for an specialized attention.
Although there are previous studies describing clinical and demographical features of dermatological patients attending emergencies departments,1–5 none of them has measured the Health Related Quality of Life (HRQL) impact in this population.
The main objective of our study was to determine how affected is the HRQL in patients with dermatological complaints evaluated in an emergency department. Also, we wanted to detect if there were differences in these scores associated with any epidemiological or clinical variable.
Patients and methodsA prospective study was performed during one month (July 2016) in the emergency department of a tertiary hospital with full-time (24h) on-call dermatologist. In total, nine different dermatology residents attended patients at the emergency department during this period. A standardized form was used to collect epidemiological and clinical information such as age, sex, marital status, level of education, diagnosis and group of diagnosis, previous visits, need of supplementary tests and discharge destination.
After every consultation, patient's self-assessment of QoL was measured using the Spanish validated versions of two self-administered questionnaires: one generic (Short-Form SF-12 Health Survey) and one specific for dermatologic patients (Dermatology Life Quality Index – DLQI). The SF-12v2 is a multidimensional 12-item instrument that includes eight domains: overall health, physical functioning, physical role, emotional role, corporal pain, mental health, vitality and social functioning. The scores in the SF-12 are standardized of 0–100 in which higher scores represent better QoL.6 The DLQI measures the impact on the QoL in a patient with a skin problem in the past 7 days.7 It has 10 questions categorized into six dimensions: symptoms and feelings (SYF), daily activities (DA), leisure (L), work or school (WS), personal relationships (PR) and treatment (T). Its scores are measured in a range of 0–30 with higher scores meaning higher impairment. This scale has been widely used in the past years in different dermatological diseases.6
Both questionnaires were offered to all adult patients visiting the emergency department with any dermatological complaint. Patients with reading or understanding difficulties, such as elderly patients, were excluded from the study. Underage patients (<18 years-old) were also excluded.
All the data were analyzed statistically using the IBM SPSS Statistics software for Windows V22.0. (Armonk, NY: IBM Corp). Kolmogorov–Smirnov test demonstrated that the scores obtained in both DLQI and SF-12v2 tests had a normal distribution. Therefore, the parametric Student's t-test was used to analyze differences between the questionnaire scores depending on variables with two categories (i.e. sex) and the analysis of variance (ANOVA) was used for those variables with more than two categories (i.e. marital status). In those cases with groups smaller than 30 patients, non-parametric Mann–Whitney U test and Kruskal–Wallis test were used. A p-value of less than 0.05 was considered as statistically significant.
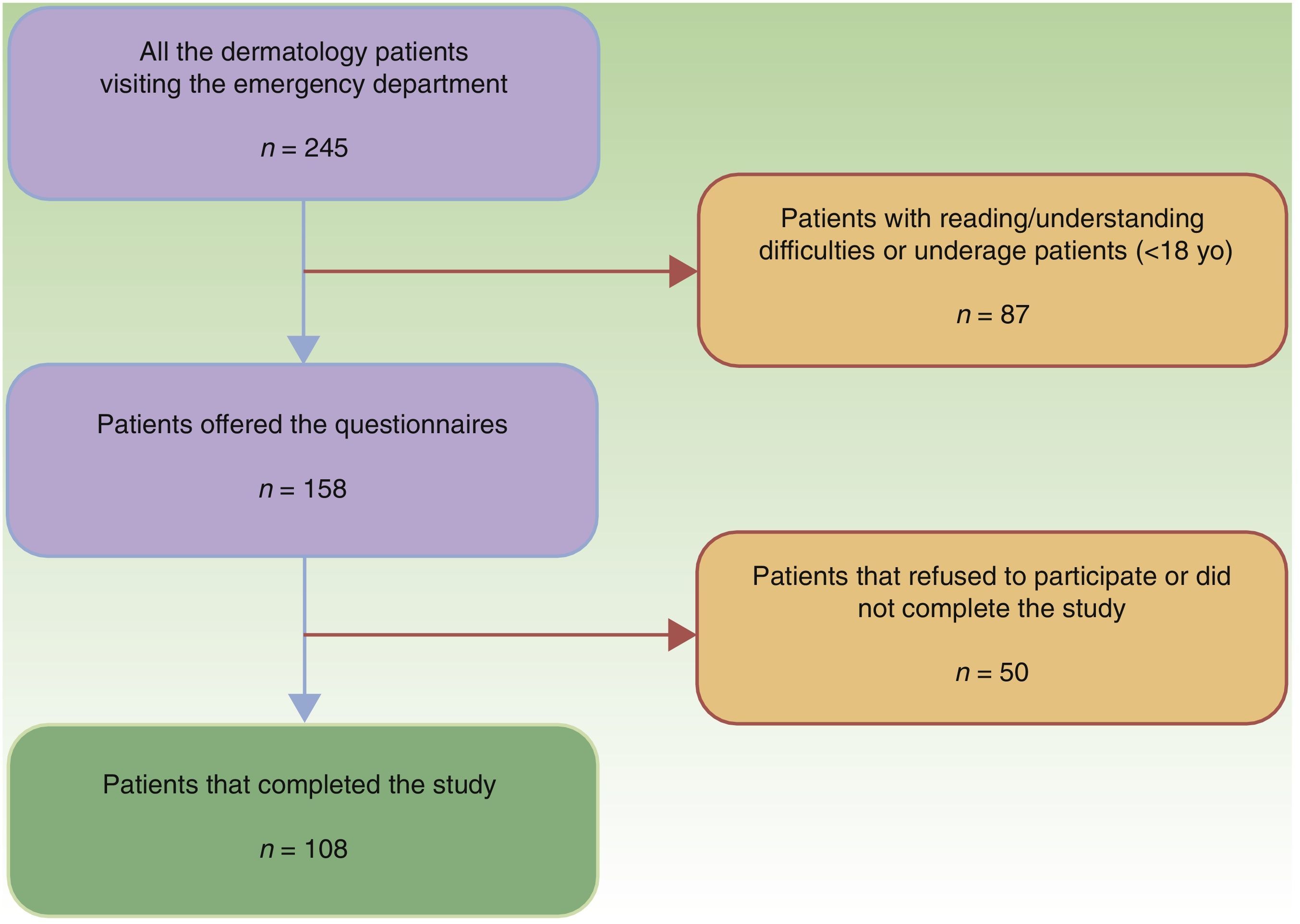
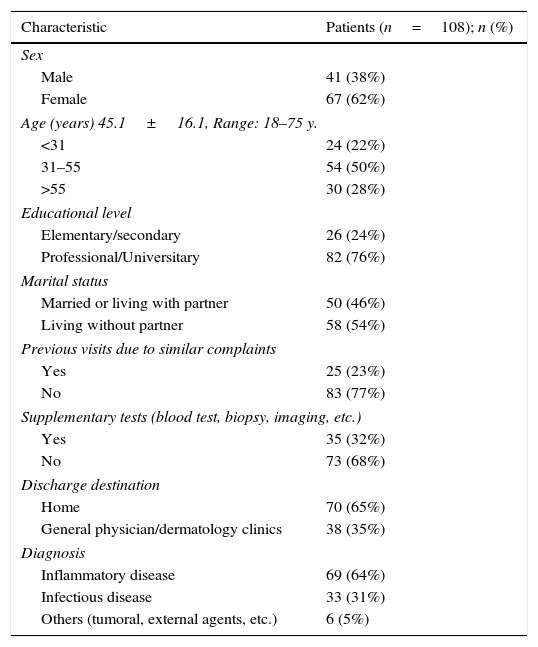
ResultsIn total, 245 patients were attended by dermatologists at the emergency department during the period of the study (mean of 8.17 patients per day). This figure represents the 3.7% of the total number of patients attended at the emergency department of the hospital on that period (6621 patients). In all, 108 patients (42.5%) met the inclusion criteria and completed both questionnaires (flow-chart of the study is represented in Fig. 1). Mean age of the studied population was 45.1 years (standard deviation: 16.1; range 18–75 years). Overall, the most common diagnoses made were urticaria (17 patients, 16%), eczema (16 patients, 14%) and infectious cellulitis (7 patients, 6%). Attending to groups of diagnoses, 69 patients (64%) had an inflammatory dermatosis; 33 patients (31%) had an infectious dermatosis and the rest of the patients (6 patients, 5%) had either a tumoral dermatosis or a post-surgical complication. The rest of the demographical and clinical features of the studied population can be found in Table 1.

Clinical and demographical features of the patients included in the study.
| Characteristic | Patients (n=108); n (%) |
|---|---|
| Sex | |
| Male | 41 (38%) |
| Female | 67 (62%) |
| Age (years) 45.1±16.1, Range: 18–75 y. | |
| <31 | 24 (22%) |
| 31–55 | 54 (50%) |
| >55 | 30 (28%) |
| Educational level | |
| Elementary/secondary | 26 (24%) |
| Professional/Universitary | 82 (76%) |
| Marital status | |
| Married or living with partner | 50 (46%) |
| Living without partner | 58 (54%) |
| Previous visits due to similar complaints | |
| Yes | 25 (23%) |
| No | 83 (77%) |
| Supplementary tests (blood test, biopsy, imaging, etc.) | |
| Yes | 35 (32%) |
| No | 73 (68%) |
| Discharge destination | |
| Home | 70 (65%) |
| General physician/dermatology clinics | 38 (35%) |
| Diagnosis | |
| Inflammatory disease | 69 (64%) |
| Infectious disease | 33 (31%) |
| Others (tumoral, external agents, etc.) | 6 (5%) |
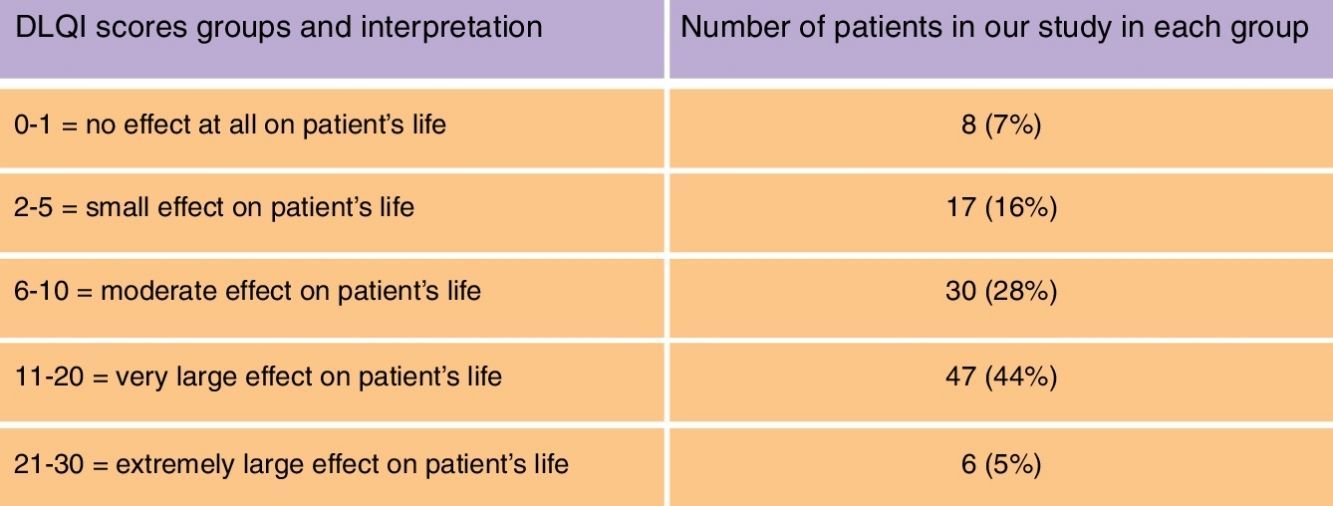
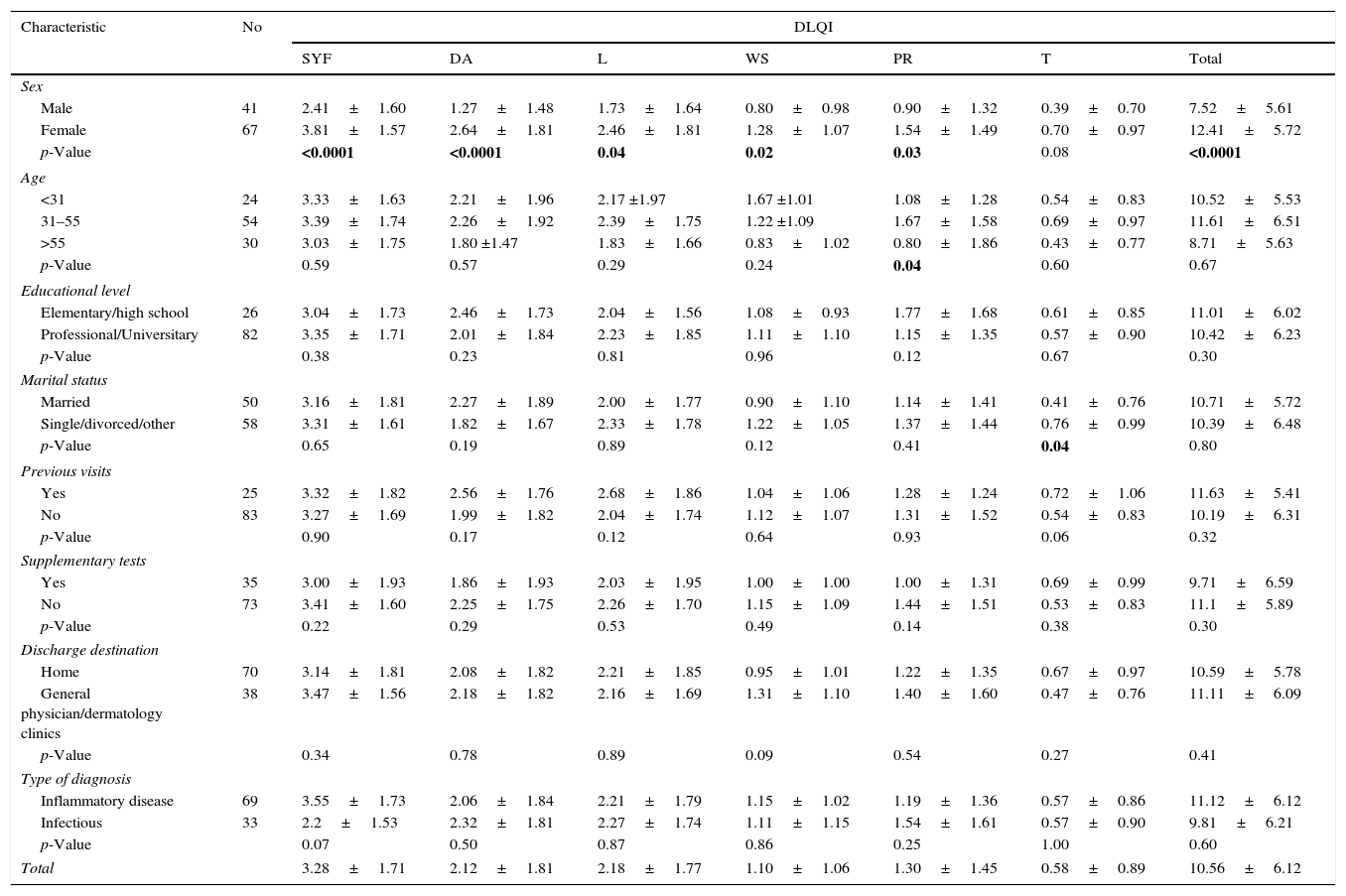
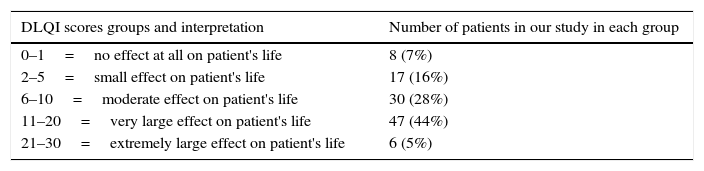
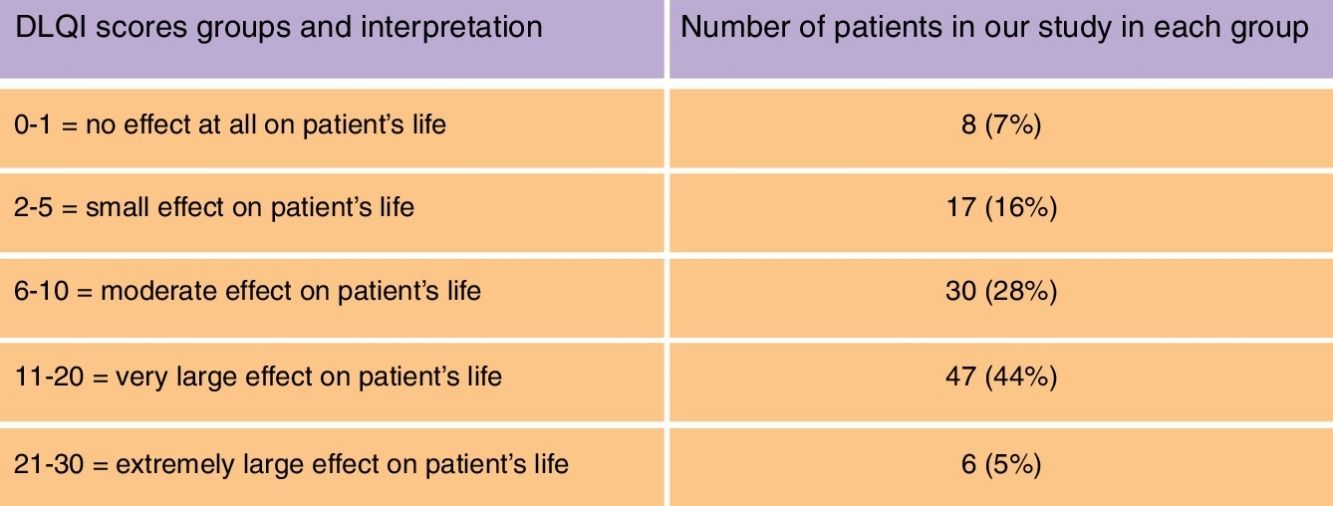
The mean DLQI score found was 10.56 (standard deviation 6.12; range 0–25). All DLQI total scores and subscale scores attending to clinical and demographical variables are detailed in Table 2. Fifty-three patients (49%) had a score of 11 or higher in the DLQI questionnaire, what is categorized as a “very large/extremely large effect on HRQL”. The number of patients on each category of the DLQI is represented in Table 3. A very significant difference (p<0.0001) was found between women's (12.4±5.7) and men's (7.5±5.6) DLQI mean score (mean difference of 4.9; 95% confidence interval of the difference: 2.7–7.1). This difference, nearly 5, is also greater to what is considered as the Minimum Clinical Important score Difference (4 points) for the DLQI. Attending to the different subscales of the DLQI depending on sex, all of the subscales except the “Treatment” item showed a statistically significant higher impairment among female patients.
Association between DLQI scores (global and subscales) and clinical variables of dermatology patients attending the emergency department.
| Characteristic | No | DLQI | ||||||
|---|---|---|---|---|---|---|---|---|
| SYF | DA | L | WS | PR | T | Total | ||
| Sex | ||||||||
| Male | 41 | 2.41±1.60 | 1.27±1.48 | 1.73±1.64 | 0.80±0.98 | 0.90±1.32 | 0.39±0.70 | 7.52±5.61 |
| Female | 67 | 3.81±1.57 | 2.64±1.81 | 2.46±1.81 | 1.28±1.07 | 1.54±1.49 | 0.70±0.97 | 12.41±5.72 |
| p-Value | <0.0001 | <0.0001 | 0.04 | 0.02 | 0.03 | 0.08 | <0.0001 | |
| Age | ||||||||
| <31 | 24 | 3.33±1.63 | 2.21±1.96 | 2.17 ±1.97 | 1.67 ±1.01 | 1.08±1.28 | 0.54±0.83 | 10.52±5.53 |
| 31–55 | 54 | 3.39±1.74 | 2.26±1.92 | 2.39±1.75 | 1.22 ±1.09 | 1.67±1.58 | 0.69±0.97 | 11.61±6.51 |
| >55 | 30 | 3.03±1.75 | 1.80 ±1.47 | 1.83±1.66 | 0.83±1.02 | 0.80±1.86 | 0.43±0.77 | 8.71±5.63 |
| p-Value | 0.59 | 0.57 | 0.29 | 0.24 | 0.04 | 0.60 | 0.67 | |
| Educational level | ||||||||
| Elementary/high school | 26 | 3.04±1.73 | 2.46±1.73 | 2.04±1.56 | 1.08±0.93 | 1.77±1.68 | 0.61±0.85 | 11.01±6.02 |
| Professional/Universitary | 82 | 3.35±1.71 | 2.01±1.84 | 2.23±1.85 | 1.11±1.10 | 1.15±1.35 | 0.57±0.90 | 10.42±6.23 |
| p-Value | 0.38 | 0.23 | 0.81 | 0.96 | 0.12 | 0.67 | 0.30 | |
| Marital status | ||||||||
| Married | 50 | 3.16±1.81 | 2.27±1.89 | 2.00±1.77 | 0.90±1.10 | 1.14±1.41 | 0.41±0.76 | 10.71±5.72 |
| Single/divorced/other | 58 | 3.31±1.61 | 1.82±1.67 | 2.33±1.78 | 1.22±1.05 | 1.37±1.44 | 0.76±0.99 | 10.39±6.48 |
| p-Value | 0.65 | 0.19 | 0.89 | 0.12 | 0.41 | 0.04 | 0.80 | |
| Previous visits | ||||||||
| Yes | 25 | 3.32±1.82 | 2.56±1.76 | 2.68±1.86 | 1.04±1.06 | 1.28±1.24 | 0.72±1.06 | 11.63±5.41 |
| No | 83 | 3.27±1.69 | 1.99±1.82 | 2.04±1.74 | 1.12±1.07 | 1.31±1.52 | 0.54±0.83 | 10.19±6.31 |
| p-Value | 0.90 | 0.17 | 0.12 | 0.64 | 0.93 | 0.06 | 0.32 | |
| Supplementary tests | ||||||||
| Yes | 35 | 3.00±1.93 | 1.86±1.93 | 2.03±1.95 | 1.00±1.00 | 1.00±1.31 | 0.69±0.99 | 9.71±6.59 |
| No | 73 | 3.41±1.60 | 2.25±1.75 | 2.26±1.70 | 1.15±1.09 | 1.44±1.51 | 0.53±0.83 | 11.1±5.89 |
| p-Value | 0.22 | 0.29 | 0.53 | 0.49 | 0.14 | 0.38 | 0.30 | |
| Discharge destination | ||||||||
| Home | 70 | 3.14±1.81 | 2.08±1.82 | 2.21±1.85 | 0.95±1.01 | 1.22±1.35 | 0.67±0.97 | 10.59±5.78 |
| General physician/dermatology clinics | 38 | 3.47±1.56 | 2.18±1.82 | 2.16±1.69 | 1.31±1.10 | 1.40±1.60 | 0.47±0.76 | 11.11±6.09 |
| p-Value | 0.34 | 0.78 | 0.89 | 0.09 | 0.54 | 0.27 | 0.41 | |
| Type of diagnosis | ||||||||
| Inflammatory disease | 69 | 3.55±1.73 | 2.06±1.84 | 2.21±1.79 | 1.15±1.02 | 1.19±1.36 | 0.57±0.86 | 11.12±6.12 |
| Infectious | 33 | 2.2±1.53 | 2.32±1.81 | 2.27±1.74 | 1.11±1.15 | 1.54±1.61 | 0.57±0.90 | 9.81±6.21 |
| p-Value | 0.07 | 0.50 | 0.87 | 0.86 | 0.25 | 1.00 | 0.60 | |
| Total | 3.28±1.71 | 2.12±1.81 | 2.18±1.77 | 1.10±1.06 | 1.30±1.45 | 0.58±0.89 | 10.56±6.12 | |
SYF, symptoms and feelings; DA, daily activities; L, leisure; WS, work and school; PR, personal relationship; T, treatment; S, symptoms; E, emotions; SF, social functioning. Bold figures serve to highlight statistically significant values.
DLQI score groups and number of patients in each group.
| DLQI scores groups and interpretation | Number of patients in our study in each group |
|---|---|
| 0–1=no effect at all on patient's life | 8 (7%) |
| 2–5=small effect on patient's life | 17 (16%) |
| 6–10=moderate effect on patient's life | 30 (28%) |
| 11–20=very large effect on patient's life | 47 (44%) |
| 21–30=extremely large effect on patient's life | 6 (5%) |
No significant differences were found in total DLQI scores associated with age, marital status, education level, diagnosis or any other variable. Significant differences were found on the “Personal relationship” subscale depending on age (p=0.04) and “Treatment” subscale depending on marital status (p=0.04).
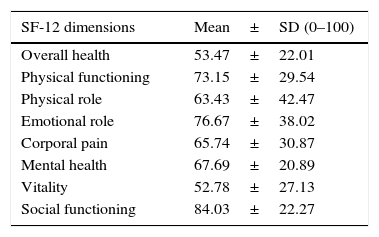
Regarding SF-12 scores, global subscale scores can be found in Table 4. The most affected dimensions in SF-12 scale were “Overall Health” (mean score of 53.47 out of 100) and “Vitality” (mean score of 52.78). Significant differences were only found in the “Social Functioning” SF-12 subscale depending on age, with lower scores in patients over 60 years old (p=0.032). There were also significantly lower scores in “Physical Functioning” and “Vitality” items among patients with lower education levels (p=0.01, p=0.04 respectively).
SF 12 mean scores in each dimension of the test.
| SF-12 dimensions | Mean±SD (0–100) |
|---|---|
| Overall health | 53.47±22.01 |
| Physical functioning | 73.15±29.54 |
| Physical role | 63.43±42.47 |
| Emotional role | 76.67±38.02 |
| Corporal pain | 65.74±30.87 |
| Mental health | 67.69±20.89 |
| Vitality | 52.78±27.13 |
| Social functioning | 84.03±22.27 |
Dermatologic diseases are rarely real life-threatening medical emergencies. However, they represent a significant percentage of the visits to emergency departments. Understanding how affected is the QoL in these patients due to the symptoms that they are experiencing is a necessary duty in order to better assess their medical problems.
The presence of an on-call dermatologist is not a constant fact in most of the hospitals in our country and general doctors attend most of the urgent cutaneous complaints. This is probably due to the general feeling among many non-dermatologist doctors that consider the skin diseases as “minor” complaints compared to other diseases attended at emergency departments.
Interestingly, the score found in our study suggests that patients visiting emergency departments with dermatological complaints have a very significant impact in their HRQL, with a mean score in the DLQI of 10.56, considered between the categories of “moderate effect (5–10)’ and “very large effect (11–20)’. In fact, 49% of the patients had a DLQI score higher than 11. This might reflect the fact that patients usually have a lot of concern when they are experiencing cutaneous acute diseases, although most of them are not considered as real medical emergencies.
Compared to the scores in usual cutaneous diseases, the mean DLQI total score in our study would be similar to that found in other studies in severe psoriasis,7 atopic dermatitis or pemphigus vulgaris8 and higher than what have been estimated for pathological scars,8 acne6 or vitiligo.9 Even though our study includes patients with different diseases, this comparison can help us to understand how intense might be the impairment that they feel.
Another interesting point is the higher impact found in female patients compared to males, of almost 5 points in total DLQI scores. The only subscale that showed no significant difference depending on sex was the “Treatment” item, probably because most of the patients included were not using any treatment at the moment of the visit. There are previous studies assessing HRQL in Dermatology that have found greater impact among women, specially those studies studying diseases with important esthetical impairment such as alopecias.10 The differences found in our study are high enough to be considered as clinically relevant. Therefore, we can assume that overall, women experiment dermatological acute symptoms with a much greater concern than males. We hypothesize whether these results are due to the more importance that women usually give to the appearance of their skin. Other possibility might be that women are more concerned about their own health. In any case, dermatologists should have this in consideration when attending this population.
Overall, the most affected subscale of the DLQI is the “Symptoms and Feeling” (SYF) dimension, with a total mean score of 3.28 (±1.71). Therefore, we can assume that the main triggers that make these patients attend emergency departments are the symptoms and the subjective concern that they feel.
A limitation of our study was that a relatively high proportion of the patients were excluded due to their age or because of reading or understanding disabilities (87 patients, 35.5% of the total population). Also a percentage of the patients included initially did not complete the questionnaires (31.6%). Another possible limitation might have been the possible impact on the HRQL due to medical or psychological comorbidities of the patients included which are sometimes associated with dermatological diseases (i.e. depression, anxiety, etc.). Also, we suggest that further studies comparing HRQL in patients with dermatological emergencies and other type of medical emergencies could provide interesting information.
Patients visiting emergency units with cutaneous complaints seem to experience a great impact on their quality of life related to the symptoms and feelings that they are living. This situation reflects the importance of attending these patients in an expeditious way, giving a correct diagnosis and a prompt treatment; a duty that can only be optimally assessed by a dermatologist.
We consider that the results of this study firmly support the presence of on-call dermatologists to better attend dermatological patients at emergencies departments. We think that it is necessary to take into account the real impact of the diseases on each patient's quality life in order to consider them as “urgent” or “non-urgent” problems.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors declare no conflict of interests.



