



The incidence of melanoma is rising in Spain. The prognostic stages of patients with melanoma are determined by various biological factors, such as tumor thickness, ulceration, or the presence of regional or distant metastases. The Spanish Academy of Dermatology and Venereology (AEDV) has encouraged the creation of a Spanish Melanoma Registry (REGESMEL) to evaluate other individual and health system-related factors that may impact the prognosis of patients with melanoma. The aim of this article is to introduce REGESMEL and provide basic descriptive data for its first year of operation.
MethodsREGESMEL is a prospective, multicentre cohort of consecutive patients with invasive cutaneous melanoma that collects demographic and staging data as well as individual and healthcare-related baseline data. It also records the medical and surgical treatment received by patients.
ResultsA total of 450 cases of invasive cutaneous melanoma from 19 participant centres were included, with a predominance of thin melanomas≤1mm thick (54.7%), mainly located on the posterior trunk (35.2%). Selective sentinel lymph node biopsy was performed in 40.7% of cases. Most cases of melanoma were suspected by the patient (30.4%), or his/her dermatologist (29.6%). Patients received care mainly in public health centers (85.2%), with tele-dermatology resources being used in 21.6% of the cases.
ConclusionsThe distribution of the pathological and demographic variables of melanoma cases is consistent with data from former studies. REGESMEL has already recruited patients from 15 Spanish provinces and given its potential representativeness, it renders the Registry as an important tool to address a wide range of research questions.
El melanoma presenta una incidencia creciente en España. Los estadios pronósticos de los pacientes con melanoma son determinados por diversos factores biológicos, como el grosor del tumor, la ulceración o la presencia de metástasis regionales o a distancia. La Academia Española de Dermatología y Venereología (AEDV) ha impulsado la creación de un Registro Español de Melanoma (REGESMEL) con el fin de evaluar otros factores de índole individual y relacionados con el Sistema Sanitario que pudieran influir en el pronóstico de los pacientes con melanoma. El objetivo de este artículo es presentar REGESMEL y proporcionar datos descriptivos básicos correspondientes a su primer año de funcionamiento.
MétodosREGESMEL es una cohorte prospectiva multicéntrica de pacientes consecutivos con melanoma cutáneo invasivo que recoge datos demográficos y de estadificación, así como datos basales individuales y relacionados con la atención sanitaria. También registra el tratamiento médico y quirúrgico recibido.
ResultadosSe incluyeron 450 casos de melanoma cutáneo invasivo procedentes de 19 centros participantes, detectando un predominio de melanomas finos con un grosor≤1mm (54,7%), localizados principalmente en el tronco posterior (35,2%). La biopsia selectiva del ganglio centinela se realizó en el 40,7% los casos. La mayoría de los casos de melanoma fueron sospechados por el propio paciente (30,4%) o por dermatólogos (29,6%). Los pacientes recibieron atención principalmente en centros sanitarios públicos (85,2%), empleándose algún recurso de teledermatología en el 21,6% de los casos.
ConclusionesLa distribución de las variables patológicas y demográficas de los casos es consistente con los datos de otros estudios. REGESMEL cuenta ya con casos de 15 provincias españolas y dada su potencial representatividad convierte el Registro en una herramienta de importancia para abordar una amplia gama de preguntas de investigación.

According to a meta-analysis conducted over the past decade, the incidence rate of cutaneous melanoma in Spain is nearly 8.7 cases per 100,000 person-years,1 which is approximately 4000 new cases each year. Recently, a possible increase in this incidence rate has been reported,2 even exceeding 2% annually.3 The mortality rate would be around 2.2 cases per 100,000 person-years.1
Currently, the prognosis of melanoma is based on variables included in the 8th edition of the American Joint Committee on Cancer (AJCC) melanoma staging,4 which are summarized in tumor thickness and ulceration for the earliest stages (stages I and II) and locoregional lymphatic involvement (lymphadenopathies and/or satellitosis), or distant metastasis for stages III and IV, each with an expected average survival.5 However, there is variability in survival within each stage, suggesting the influence of other less studied factors, in addition to the biological characteristics of the tumor. In Sweden, an impact of socioeconomic factors in this regard has been reported,6 but the possible influence of these factors in Spain is unknown to this date. Furthermore, assessing whether there are individual-related factors (demographic, socioeconomic, clinical) as well as factors related to health care in Spain that may imply diagnostic delays could provide highly relevant information for improving the survival of melanoma-diagnosed patients in the future, by identifying vulnerable populations and potential areas for improvement in health care.
To address these issues, it is essential to have a melanoma patient registry that is as representative as possible both geographically and in terms of different types of health care. The Spanish Academy of Dermatology and Venereology (AEDV) has spearheaded the creation of such a registry, known as the Spanish Melanoma Registry (REGESMEL).
The aim of this article is to present REGESMEL, and provide basic descriptive data in its first year of operation.
Materials and methodsDesignThis is a prospective cohort that collects pseudonymized data of consecutive patients with new diagnoses of invasive primary cutaneous melanoma. Melanomas in situ, mucosal melanomas (except for those located in the genital area that do not affect the mucosa), and melanomas of unknown origin are excluded from the study.
Measurement and variablesStudy data are collected and managed using the Research Electronic Data Capture (REDCap) electronic data capture tools hosted at the AEDV.7 REDCap is a secure web-based software platform designed to support data capture for research studies.
The study was approved by Hospital Universitario Reina Sofía Clinical Research and Ethics Committee, Córdoba, Spain (reference No.: 5345). The study includes an early visit and further follow-up visits in which data are collected in 4 blocks: a) Inclusion, covering demographic data (including place of residence), skin phototype, primary tumor details, and data on initial staging; b) Baseline and detection status describing the patients’ history, their personal situation, and aspects related to lesion diagnosis by the patient or the health care system; c) Surgical procedure performed; d) Medical treatment, without specifying doses or intervals.
During follow-up visits, tests performed, information on staging, and the patient's vital status are collected. A section on second or subsequent melanomas is also included, detailing their staging (see Appendix A of the supplementary data).
For this study, collected data have been compiled into indices based on the nature of the variable (mean and standard deviation, frequencies, medians).
REGESMEL incorporates information on the patients’ approximate residence obtained through the Cartociudad portal of the Government of Spain,8 from which the patients’ census residence is obtained. This information will allow drawing information on the patients’ socioeconomic level (based on the Spanish deprivation index developed by the Spanish Society of Epidemiology9) and type of residential environment (urban or rural) using spatial analysis techniques. The census record, province, and autonomous community of residence will be the units of analysis.
For this initial work, basic descriptive data include a few individual-related factors (such as age, sex, functional status, province of residence), tumor biology-related factors (Breslow tumor thickness, stage, and location), and finally health care-related factors (such as the type of health center involved, the person who established the level of suspicion, the use of teledermatology tools, and whether selective sentinel lymph node biopsy (SLNB) was performed).
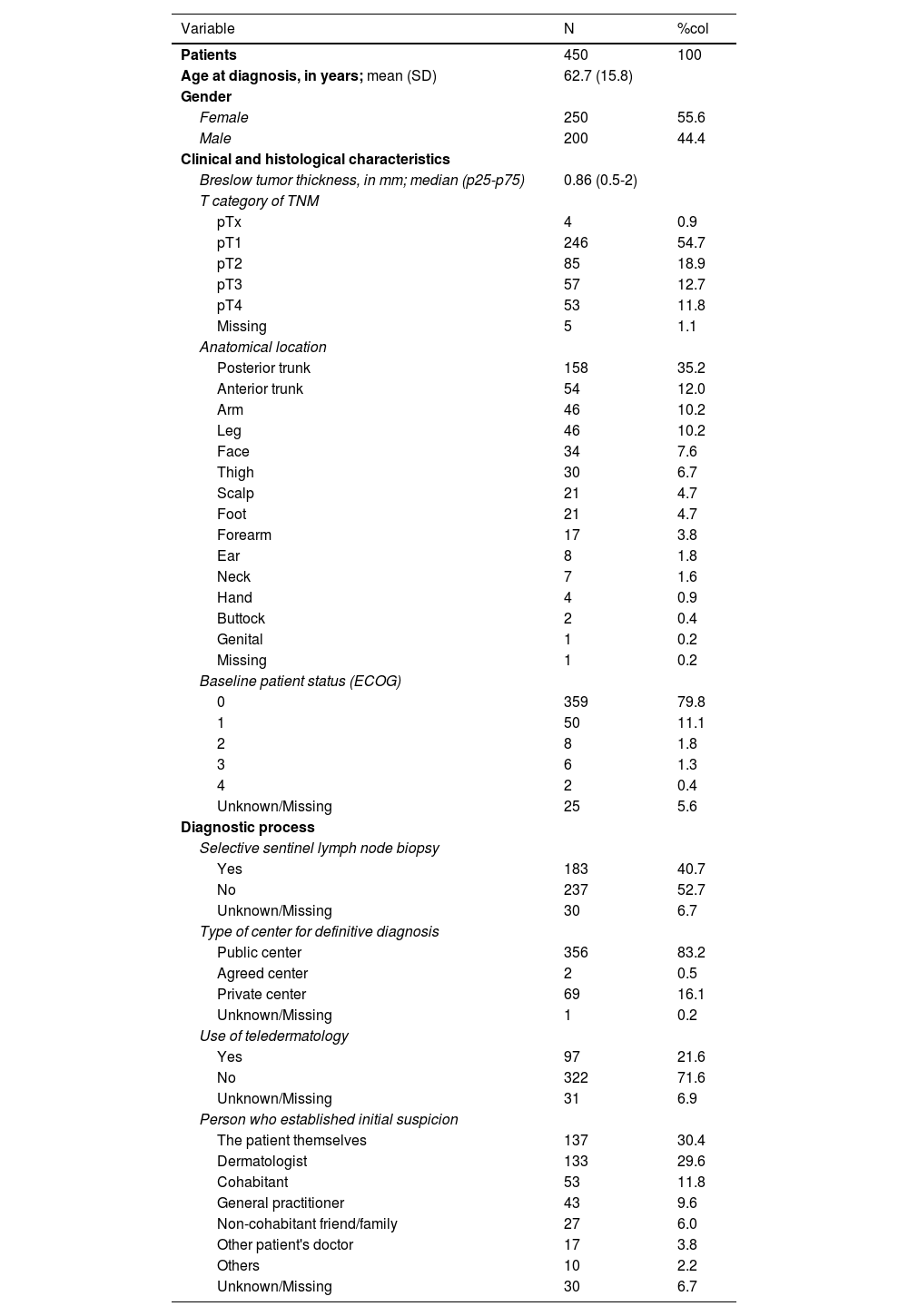
ResultsThe Registry began to include patients on June 1st, 2022, with the progressive inclusion of different participant centers. At the time of analysis, September 30th, 2023, the registry included a total of 450 patients from 19 hospital centers across Spain (see table 1). Regarding gender distribution, 250 patients (55.6%) were women and 200 (44.4%) men, with a mean age of 62.7 (SD, 15.8). Figure 1 shows the distribution by provinces, with Barcelona and Madrid contributing the highest number of cases (25.3% and 23%, respectively).
Characteristics of REGESMEL patients within its first year of operation.
| Variable | N | %col |
|---|---|---|
| Patients | 450 | 100 |
| Age at diagnosis, in years; mean (SD) | 62.7 (15.8) | |
| Gender | ||
| Female | 250 | 55.6 |
| Male | 200 | 44.4 |
| Clinical and histological characteristics | ||
| Breslow tumor thickness, in mm; median (p25-p75) | 0.86 (0.5-2) | |
| T category of TNM | ||
| pTx | 4 | 0.9 |
| pT1 | 246 | 54.7 |
| pT2 | 85 | 18.9 |
| pT3 | 57 | 12.7 |
| pT4 | 53 | 11.8 |
| Missing | 5 | 1.1 |
| Anatomical location | ||
| Posterior trunk | 158 | 35.2 |
| Anterior trunk | 54 | 12.0 |
| Arm | 46 | 10.2 |
| Leg | 46 | 10.2 |
| Face | 34 | 7.6 |
| Thigh | 30 | 6.7 |
| Scalp | 21 | 4.7 |
| Foot | 21 | 4.7 |
| Forearm | 17 | 3.8 |
| Ear | 8 | 1.8 |
| Neck | 7 | 1.6 |
| Hand | 4 | 0.9 |
| Buttock | 2 | 0.4 |
| Genital | 1 | 0.2 |
| Missing | 1 | 0.2 |
| Baseline patient status (ECOG) | ||
| 0 | 359 | 79.8 |
| 1 | 50 | 11.1 |
| 2 | 8 | 1.8 |
| 3 | 6 | 1.3 |
| 4 | 2 | 0.4 |
| Unknown/Missing | 25 | 5.6 |
| Diagnostic process | ||
| Selective sentinel lymph node biopsy | ||
| Yes | 183 | 40.7 |
| No | 237 | 52.7 |
| Unknown/Missing | 30 | 6.7 |
| Type of center for definitive diagnosis | ||
| Public center | 356 | 83.2 |
| Agreed center | 2 | 0.5 |
| Private center | 69 | 16.1 |
| Unknown/Missing | 1 | 0.2 |
| Use of teledermatology | ||
| Yes | 97 | 21.6 |
| No | 322 | 71.6 |
| Unknown/Missing | 31 | 6.9 |
| Person who established initial suspicion | ||
| The patient themselves | 137 | 30.4 |
| Dermatologist | 133 | 29.6 |
| Cohabitant | 53 | 11.8 |
| General practitioner | 43 | 9.6 |
| Non-cohabitant friend/family | 27 | 6.0 |
| Other patient's doctor | 17 | 3.8 |
| Others | 10 | 2.2 |
| Unknown/Missing | 30 | 6.7 |
SD, standard deviation.

Regarding anatomoclinical data, thin melanomas ≤ 1mm constituted the majority group (54.7%) (table 1). The most frequent locations were posterior trunk (35.2%), anterior trunk (12%), arm (10.2%), and leg (10.2%).
Regarding health care-related factors, 83.2% of patients received treatment at a public center, 16.1% at a private center, and 0.5% at a public-private partnership center, with access covered by the public health care system. Additionally, some form of teledermatology mechanism was used in 21.6% of cases.
A total of 40.7% out of the total number of patients included underwent SLNB, 173 of patients (67.6%) with ≥ pT1b and 10 patients (5%) with pT1a. Most cases had good functional status (79.8% had ECOG 0 functional status; and 11%, ECOG 1).
Regarding the person who suspected diagnosis, in one-third of cases (30.4%), it was the patient themselves, while in another third, the dermatologist (29.6%) did so followed by cohabitants (11.8%) or the general practitioner (9.6%).
DiscussionThe REGESMEL registry, promoted by the AEDV, is a novel project with different objectives from the previous melanoma registry developed by the AEDV.10
In its first year of operation, REGESMEL has been well received among Spanish academic dermatologists with participation from 19 centers and the inclusion of more than 400 patients. Considering the estimated incidence rate in Spain (between 3600 and 4700 new cases each year1), the inclusion of almost 10% of cases within the first year reflects good prospects for achieving significant population representativeness, despite 30 provinces still lacking centers linked to the project.
To date, the disease is more prevalent among women, representing 55.6% of cases, very similar to previous data in our country,10 which contrasts with data from southern Europe where more cases are diagnosed in men.11
Regarding the Breslow tumor thickness, we should mention that 54.7% of all melanomas reported are thin melanomas ≤ 1mm. This information updated to 2023 reflects a constant trend of increasingly thinner lesions diagnosed vs the 46.7% reported from 1997 through 2001, the 50.8% reported from 2002 through 2006, and the 53.3% described form 2007 through 2011.10 This increase in thin lesions is a trend observed across Europe.12
The most common location of melanomas is the posterior trunk, accounting for 35.2% of cases, and together with the anterior trunk (12%), they account for 47.2%. On the other hand, locations in arms, legs, or thighs comprise approximately 10% of cases or even less. Head and neck areas account for <10% in each of their sublocations, such as face, scalp, ear, and neck. This data is relevant for several reasons. Firstly, it can help support etiopathogenic hypotheses related to intermittent exposure to UV radiation vs chronic exposure in the head and neck region. Moreover, it has significant implications for education and screening practices, since nearly half of the cases are diagnosed on the trunk, suggesting the importance of recommending examination of the back and anterior trunk, according to each patient's risk profile.13
Most patients (83.2%) received a definitive diagnosis at public health care centers, while in private centers, this rate was 16.1% (dropping to 0.5% in centers with agreements). This suggests that the presence of private centers in REGESMEL would be represented based on the reality of Spain14 since, according to data from the Spanish National Institute of Statistics, 16.3% of the population has private health care insurance.15
A striking data is that in 21.6% of registered melanoma cases, some form of teledermatology tool was used in their management. This reflects the current increasing use of various teledermatology tools in skin cancer diagnosis and makes the registry a highly interesting element in the coming future to evaluate different variables related to teledermatology in Spain.16
In the Registry, 30.4% of cases were initially suspected by the patients themselves, followed by 29.6% of cases which were suspected by dermatologists. These data are different from those published back in 2016 by Avilés-Izquierdo et al.17 (53% and 20%, respectively). Recent studies on self-detection of cutaneous cancer by patients provide similar results (50% self-detection), also highlighting the importance of the patients’ environment in suspicion of cutaneous tumors.18,19
The SLNB was performed in 40.7% of all reported cases. Clinical practice guidelines recommend discussing and offering SLNB to patients with melanoma ≥ pT1b.20,21 These melanomas encompass 46.7% of all reported cases (data not shown), which means that the percentage of SLNB performance in Spain seems to be higher than that reported in other countries such as Australia or the United States.22,23
The incorporation of geographical data into cancer studies is becoming increasingly important24 and can provide relevant information in the field of melanoma.25,26 REGESMEL allows analyzing geographical data at census tract level and already has active recruitment in 15 Spanish provinces. Several centers from other provinces are about to start their participation, and efforts will be made to continue adding other areas within Spain.
In conclusion, some preliminary data from REGESMEL within its first year of operation have been presented. The distribution of pathological and demographic variables shown is consistent with data provided by other studies. Additionally, the number of included patients and their potential representativeness, estimated in relation to the total number of diagnosed melanoma patients in Spain, makes the registry an important tool for addressing a wide range of research questions. These are not only limited to those related to melanoma biology and its management but also involve various individual patient factors and the health care system per se in relation to the prognosis of this type of tumor. Studying these factors could help identify vulnerable population groups in Spain and create a window of opportunity to implement public health measures aimed at strengthening areas where intervention is most needed.
As a result, REGESMEL has become a valuable research tool available to AEDV academics who want to collaborate through their work centers or propose their own research projects.
FundingREGESMEL has received untied support for its implementation from ISDIN S.A. (Barcelona, Spain).
Conflicts of interestSusana Puig has been a speaker for: Almirall, Cantabria, Eucerin, ISDIN, La Roche Posay, Novartis, Pierre Fabre, Roche, Sanofi, Sunpharma; consultant or advisory board member for: Almirall, BMS, Biofrontera, MSD, ISDIN, La Roche Posay, Novartis, Polychem, Sunpharma. GRANTS & RESEARCH SUPPORT: Almirall, Amgen, AMLO, BMS, Biofrontera, Canfield, Cantabria, Castle Bioscience, Eucerin, Fotofinder, GSK, ISDIN, La Roche Posay, Leo, Mavig, Novartis, Polychem, Roche, Edposo/partner: Almirall, Amgen, BMS, Canfield, Fotofinder, ISDIN, La Roche Posay, Mavig, Nevisense, Novartis, Pierre Fabre, Roche. Others: Abbie (educational activities), Lilly (educational activities), co-founder of Diagnosis Dermatologica sl and Athena Tech, investor of Dermavision.
The remaining authors declared no conflicts of interest whatsoever.
REGESMEL group members: Marcial Álvarez-Salafranca (Hospital Universitario Miguel Servet, Zaragoza, Spain), María Navedo de las Heras (Complejo Asistencial Universitario de León, León, Spain), Martina Espasandín Arias (Complejo Hospitalario Universitario de Pontevedra, Spain), Marta Bertolín-Colilla (Hospital del Mar, Barcelona, Spain), Lula María Nieto Benito (Clínica Universidad de Navarra, Madrid, Spain) María Huerta Brogeras (Clínica Universidad de Navarra, Madrid, Spain).



