



Ingrown nails or onychocryptosis is an inflammatory disease that, according to classic literature, is caused by compression of the nail against the lateral and distal periungual edges. It is a very common process that most frequently affects the big toe and is seen especially in young or adolescent patients with inappropriate footwear or mis-trimming of the nail. Usual treatment in persistent cases normally involves surgery, with different options involving the nail and nail matrix (matricectomy and partial nail avulsion) or removal of the edematous, granulomatous, or hypertrophic periungual tissue.
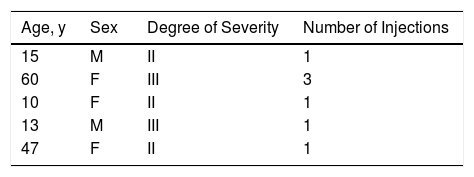
We report 5 cases of ingrown nails treated with intralesional injection of corticosteroids as adjuvant or reducing treatment prior to surgical intervention. We initially staged the severity of the condition using the Heifetz scale. In all cases, intralesional injections of 0.5-1mL of a 40mg/mL commercial solution of triamcinolone acetonide, diluted at a ratio of 1:5 in an anesthetic solution of mepivacaine 2%, were administered along the inflamed edge of the fold. Five patients (2 male and 3 female) aged between 10 and 60 years were treated. Three cases were moderate (stage II) and 2 were severe (stage III). In 4 of these patients, a single injection was sufficient to resolve the problem and avoid surgical intervention; in another patient, in light of the success of the previous cases, we decided to repeat the injection twice, with an interval of 3 weeks, and surgical intervention was also avoided (Table 1). All the patients responded satisfactorily with disappearance of inflammation and substantial improvement of pain (Figs. 1 and 2). The patients were advised to make major changes in the use of footwear, including adapting it as much as possible to suit their feet, avoiding or limiting the use of excessively high heels, wearing open footwear in summer and switching from the use of boots or shoes outdoors to slippers in the home. No relapse was observed during follow-up of the patients (between 6 months and 3 years).


To date, ingrown nails have been treated almost exclusively with surgery, removing the nail segment embedded in the laterodistal nail bed and/or reducing the hypertrophic tissue to widen the nail bed and allow the nail to grow without embedding. Although local treatments and conservative techniques (such as external nail splints, use of dental floss, cotton, or surgical tape to separate the nail from the nail bed) may alleviate or temporarily resolve the discomfort and complications caused by ingrown nails, in most cases, patients eventually undergo surgery, even in mild cases.1 Some authors propose chemical matricectomy with phenol as the treatment of choice in initial stages (stages I and II); relapse after this treatment ranges between 8% and 17%.2 Other surgical techniques aim to minimize surgical aggression. These include placing a splint between the nail bed and the nail so that the nail grows over the fold without re-embedding (tube technique) or eliminating the hypertrophic tissue and suturing under the nail (knot technique).3,4 In more severe stages, in which the nail is almost completely embedded under the nail fold, surgery tends to be more complex and requires resection of more hypertrophic tissue (Winograd, Dubois, or super U technique), which leads to greater postoperative morbidity.5 In all these cases, the morbidity due to nail surgery, such as pain, bleeding, and infection, may be significant, as are the limitations in some types of patient with circulatory problems, such as diabetic patients or smokers, owing to potential ischemia.6
Most cases of ingrown nails reveal clear use of inappropriate footwear (both in length and, especially, in width). The condition more often affects overweight patients, patients with poor foot care, and adolescents who excessively use closed footwear on rapidly growing feet. The resulting compression in all these cases causes inflammation of the periungual fold, which is pushed against the edge of the nail, initiating a vicious circle of inflammation-edema-embedding and more inflammation.
Intralesional corticosteroids are widely used in different skin diseases and dermatologists are familiar with their use in other indications.7,8 As has been seen in the patients reported here, treating ingrown nails with injections of depot corticosteroids along the involved nail fold is a simple, conservative option that can be applied in the consulting rooms and that makes it possible to avoid much probably unnecessary surgery and frequent relapse of a dermatologic problem with associated morbidity.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Vílchez-Márquez F, Morales-Larios E, Torre EdRdl. Tratamiento no quirúrgico de las uñas encarnadas con infiltración local de triamcinolona Eczema y urticaria en Portugal. 2019;110:772–773.



