



We report the case of a previously healthy 51-year-old male patient that presented with a twelve-month history of skin lesions located at the trunk. The lesions caused local burning and were exacerbated by heat and sweating. There were no associated cutaneous or extracutaneous symptoms and the patient denied any relevant family history. On physical examination, there were multiple grouped erythematous keratotic papules and erosions in a blaschkoid distribution on the trunk (Fig. 1). The patient had no mucosal or nail lesions.

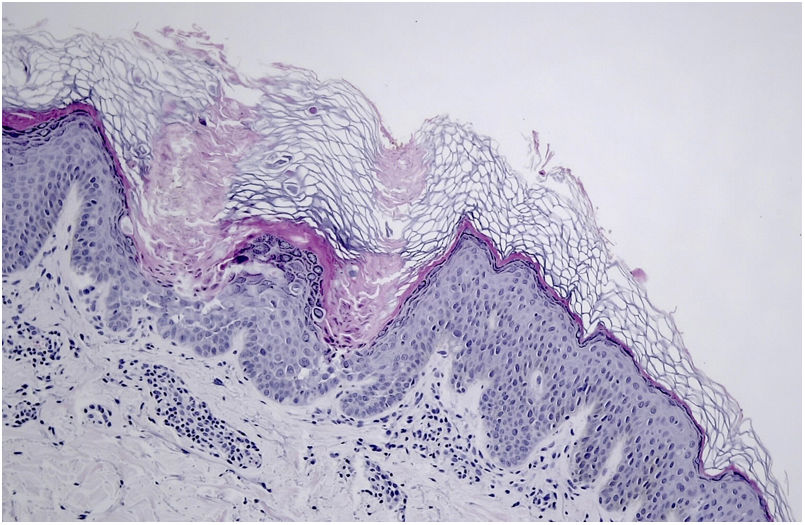
Lesional biopsy revealed multiple foci of acantholysis and dyskeratosis, grains and occasional corps ronds (Fig. 2).
What is the diagnosis?
DiagnosisSegmental Darier Disease (type 1).
CommentsDarier disease is an autosomal dominant genodermatosis, characterized by the presence of mutations in the ATP2A2 gene. These mutations result in dysfunction of an endoplasmic reticulum Ca2+ ATPase (SERCA2), thus interfering in the signaling of intracellular calcium. Consequently, there is loss of supra-basal cell adhesion (acantholysis) and induction of apoptosis (dyskeratosis).
From a clinical point of view, classic Darier disease is characterized by the presence of crusted greasy keratotic papules and plaques, located predominantly in seborrheic areas. Additional findings include palmoplantar papules, whitish papules on the oral mucosa and variable nail changes, including V-shaped notching and alternating white and red longitudinal streaks, which is considered pathognomonic.1 Environmental factors, including heat, friction, sweating and UV light can induce flares, and some medications are also known to cause exacerbations, namely lithium.2 Darier disease follows a chronic course with oscillations in disease severity and secondary bacterial and viral infections are frequent complications.
In addition to the more classic presentation, two types of segmental Darier disease have been described, both with lesions distributed along the lines of Blaschko. The most common subtype is type 1, which is the result of a post-zygotic mutation in the ATP2A2 gene during embryogenesis, thus prompting cutaneous mosaic involvement. In type 1 segmental disease, the age of onset, severity and histological findings are similar to the generalized Darier form. Type 2 mosaicism is more severe and less frequent. These patients present with generalized Darier disease as well as additional linear lesions, with increased severity.3 Type 2 segmental disease occurs when patients carrying a heterozygous germline mutation have an additional postzygotic inactivating mutation in the other allele of the same gene, causing loss of heterozygosity. The histological findings described in this patient evoke the diagnosis of Darier's Disease; in light of the clinical picture described, this case corresponds to type 1 segmental disease.
The therapeutic approach to Darier disease is often difficult and challenging. General measures including avoidance of heat and minimization of friction are helpful.2 In addition, corticosteroids can be used to reduce inflammation and topical antimicrobial washes may help decrease the risk of superimposed infection. Systemic retinoids and low-dose naltrexone have been used in some cases with good results.2 Surgical approach is an option in severe refractory cases. Our patient was started on acitretin 10mg daily with marked improvement and remains under surveillance.
The clinical differential diagnosis of type 1 segmental Darier disease includes Blaschkoid linear acquired inflammatory skin eruption, linear lichen planus, linear porokeratosis and nevus unis lateris. Histopathology findings are of major importance, establishing the diagnosis. Early diagnosis will help avoid unnecessary and costly treatment for unrelated conditions.
Conflict of interestsThe authors declare that they have no conflict of interest.



