



The majority of onychomycoses are caused by dermatophytic fungi or yeasts; those due to nondermatophyte molds account for approximately 10% worldwide, with different sources reporting between 1.45% and 17.6%.1,2 However, numerous nondermatophyte filamentous fungi are often isolated as commensals from pathologic nails, mainly from the toenails of persons of advanced age.3
A 64-year-old woman with diabetes mellitus consulted for a 2-month history of discoloration of the nail and nail bed of her left great toe. She denied trauma but did describe a previous episode of periungual inflammation.
Physical examination revealed onychoclasis and onychomadesis with black discoloration of the proximal nail bed and marked dystrophy of the nail plate (Fig. 1A). Hutchinson sign was negative and dermoscopy did not reveal a micro-Hutchinson sign.

The differential diagnosis included subungual melanoma and infection, and microbiology examination of the nail was therefore requested. Culture was positive for Aspergillus niger (Fig. 2), and the search for dermatophytes and bacterial culture was negative. Based on these findings, we made a diagnosis of proximal subungual onychomycosis due to A. niger. Treatment was started with 40% urea and bifonazole cream under an occlusive dressing, leading to a progressive clinical improvement. At 5 months the pigmentation had practically disappeared, leaving a residual partial anonychia (Fig. 1B); cultures were negative.

Onychomycosis due to nondermatophyte molds is difficult to diagnose, as these organisms are common contaminants of diseased nails.1 In contrast to the dermatophytes, Aspergillus spp. is a nonkeratophilic fungus that usually causes secondary infection in nails damaged by trauma or previous disease.3,4 However, both Aspergillus and other molds are an emerging cause of onychomycosis, mainly affecting the toenails of diabetic patients.5,6 The apparent increase in the incidence of this type of infection could be due to aging of the population, better diagnostic techniques, or increased awareness of the pathogenic capacity of these organisms.4,5 Other nondermatophyte filamentous fungi associated with nail disease include Scopulariopsis brevicaulis, Acremonium spp., and Fusarium spp.1,4
The clinical presentation of onychomycosis due to molds can be very variable, and the diagnosis cannot be established on clinical criteria alone.3 In the literature, it has been indicated that A. niger can be associated with periungual inflammation, brown-to-black pigmentation, or even striate melanonychia.4,7–9
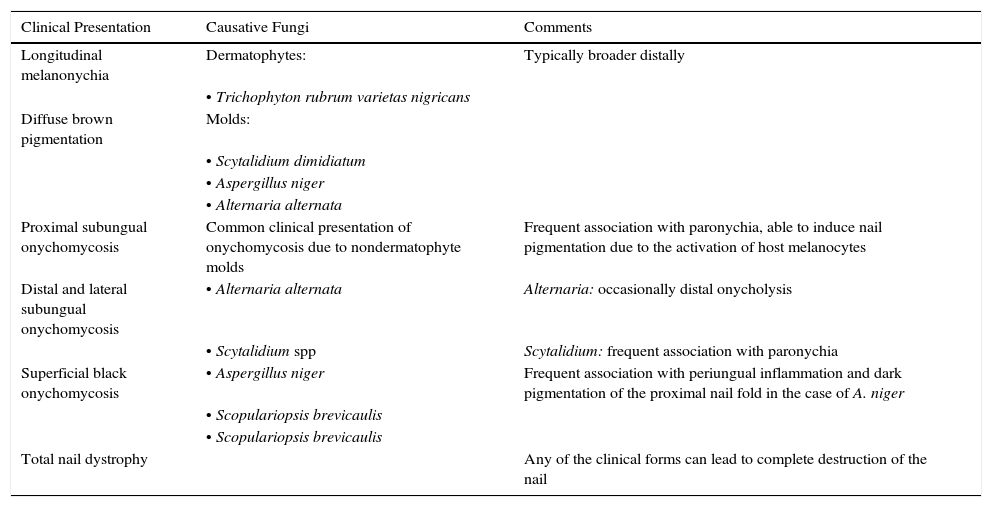
Melanonychia of fungal origin with brown or black pigmentation of the nail unit is relatively rare and can mimic subungual melanoma (Table 1).7 It is more common in men, in older adults, and in the toenails. The majority of cases are due to dematiaceous or melanin-producing fungi, with the most common being Scytalidium dimidiatum and Alternaria spp.7A. niger is a nondematiaceous fungus, whose dark color is due to aspergillin pigment, which can make the nail and proximal nail fold dark brown or black.7
Clinical Presentation of Melanonychia of Fungal Origin.
| Clinical Presentation | Causative Fungi | Comments |
|---|---|---|
| Longitudinal melanonychia | Dermatophytes: | Typically broader distally |
| • Trichophyton rubrum varietas nigricans | ||
| Diffuse brown pigmentation | Molds: | |
| • Scytalidium dimidiatum | ||
| • Aspergillus niger | ||
| • Alternaria alternata | ||
| Proximal subungual onychomycosis | Common clinical presentation of onychomycosis due to nondermatophyte molds | Frequent association with paronychia, able to induce nail pigmentation due to the activation of host melanocytes |
| Distal and lateral subungual onychomycosis | • Alternaria alternata | Alternaria: occasionally distal onycholysis |
| • Scytalidium spp | Scytalidium: frequent association with paronychia | |
| Superficial black onychomycosis | • Aspergillus niger | Frequent association with periungual inflammation and dark pigmentation of the proximal nail fold in the case of A. niger |
| • Scopulariopsis brevicaulis | ||
| • Scopulariopsis brevicaulis | ||
| Total nail dystrophy | Any of the clinical forms can lead to complete destruction of the nail |
The diagnostic criteria of onychomycosis due to nondermatophyte molds are not well-established. In general, 6 major criteria suggest the pathogenic nature of the nondermatophyte fungus (observation on direct examination, positive culture, repeated isolation, inoculum count, the exclusion of dermatophyte fungi, and histology), with 3 criteria being necessary to exclude simple colonization.1 Our patient satisfied 2 criteria (positive culture and the exclusion of a dermatophyte), but histology and the inoculum count were not performed. The very characteristic melanonychia was suggestive of A. niger as the causative agent.
The differential diagnosis of fungal melanonychia should include subungual hematoma, racial pigmentation, drug-induced melanonychia, exogenous pigmentation, and melanocyte hyperplasia, including subungual melanoma.7
The treatment of onychomycosis due to molds is often unsatisfactory.2,3 The onychomycoses associated with global nail pigmentation are considered difficult to treat.7A. niger, on the other hand, has shown a good response to topical ciclopirox, oral terbinafine, and oral itraconazole.1,2,4,7,10 Photodynamic therapy with methyl aminolevulinate and other photosensitizers has also been shown to be effective in the treatment of some nondermatophyte molds, and can be considered in cases with a poor response to conventional treatments,11 but the presence of pigment, as in our case, could affect efficacy.
In conclusion, we have presented a case of proximal subungual onychomycosis due to A. niger. Despite its low frequency, its characteristic clinical presentation means this infectious agent must be taken into account in the differential diagnosis of pigmented nail dystrophy. In these cases, the differential diagnosis should always include malignant melanoma, and biopsy should be considered in case of doubt.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Álvarez-Salafranca M, Hernández-Ostiz S, Salvo Gonzalo S, Ara Martín M. Onicomicosis subungueal proximal por Aspergillus niger: un simulador de melanoma maligno subungueal. Actas Dermosifiliogr. 2017;108:481–484.



