


Lichen sclerosus (LS) is a chronic inflammatory mucocutaneous disease1 that has a huge impact on the patients’ quality of life.2 Ultrapotent topical corticosteroids (UPTC) do not always control symptoms and have been associated with deleterious local adverse effects,3 which exacerbates LS symptoms. Other non-invasive approaches such as photodynamic therapy (PDT) or laser therapy yield promising results.3,4 However, as far as we know, the combination of the two has never been reported to this date.
We conducted a descriptive retrospective analysis on patients on combined therapy with fractional microablative CO2 laser (FMCL) and PDT for refractory LS in two different dermatology departments. Therapy was administered as an outpatient procedure under topical anesthesia, although this modality could modify further drug absortion. Initially, we performed FMCL over the treatment area using two CO2 laser devices depending on the availability of each center (Table 1), followed by the administration of 1g of 5-aminolevulinic acid 78mg/g (Ameluz®, Biofrontera, Leverkusen, Germany) for every 25cm2 of affected skin placed under occlusion for 90min. Afterwards, the patient was positioned to expose the maximum affected area (e.g. with legs abducted and flexed to expose the genital area) which was then exposed to the PDT lamp BF-RhdoLED® (Biofrontera) for 20min (wavelength 630nm, light dose 37Jcm−2). If necessary, treatment was readministered after a 6-week interval. Disease activity was assessed using the Investigator's Global Assessment (IGA, 0–3), and the LS-related pain was rated using a visual analogue scale (VAS, 0–10). Patients were also asked about their pain during sexual activity. These assessments were conducted before and 3 months after therapy. Patient satisfaction with the procedure was rated from 0 to 100. Pre- and post-treatment results were compared using the paired-sample Wilcoxon test. This study was approved the Ethical Board, and all patients signed the corresponding written informed consent form.
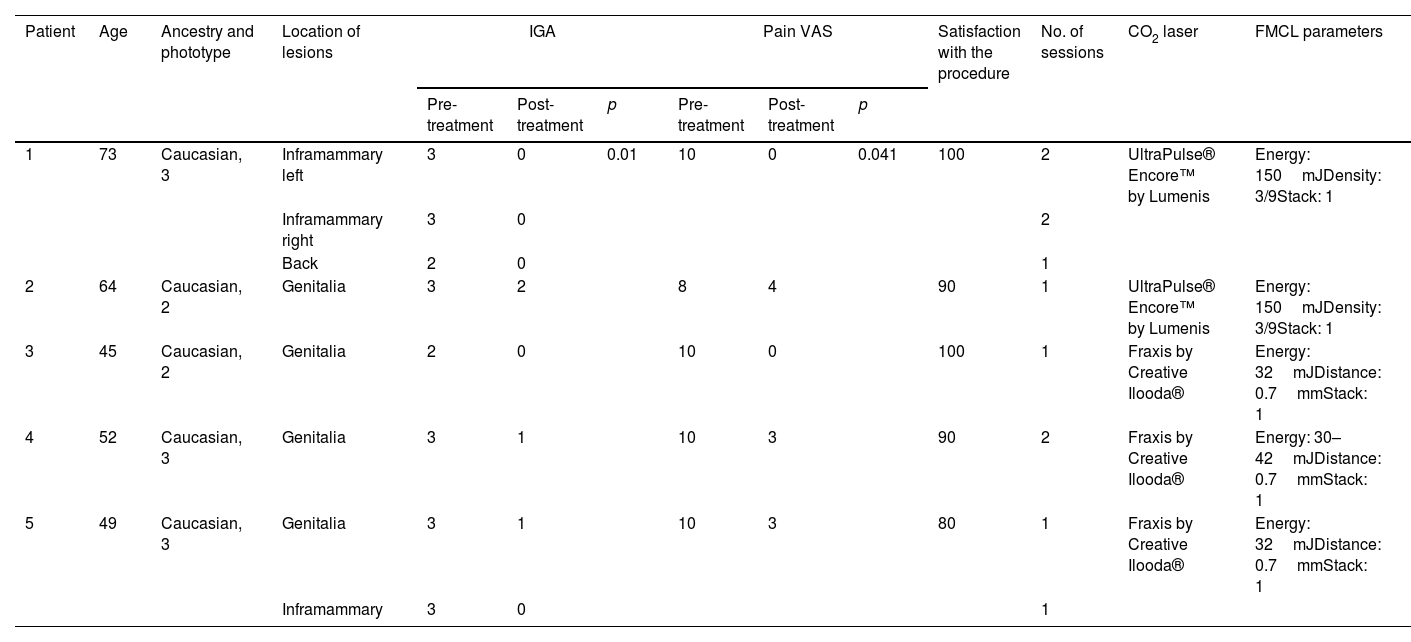
Summary of the patients’ characteristics and outcomes and lasers used.
| Patient | Age | Ancestry and phototype | Location of lesions | IGA | Pain VAS | Satisfaction with the procedure | No. of sessions | CO2 laser | FMCL parameters | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-treatment | Post-treatment | p | Pre-treatment | Post-treatment | p | ||||||||
| 1 | 73 | Caucasian, 3 | Inframammary left | 3 | 0 | 0.01 | 10 | 0 | 0.041 | 100 | 2 | UltraPulse® Encore™ by Lumenis | Energy: 150mJDensity: 3/9Stack: 1 |
| Inframammary right | 3 | 0 | 2 | ||||||||||
| Back | 2 | 0 | 1 | ||||||||||
| 2 | 64 | Caucasian, 2 | Genitalia | 3 | 2 | 8 | 4 | 90 | 1 | UltraPulse® Encore™ by Lumenis | Energy: 150mJDensity: 3/9Stack: 1 | ||
| 3 | 45 | Caucasian, 2 | Genitalia | 2 | 0 | 10 | 0 | 100 | 1 | Fraxis by Creative Ilooda® | Energy: 32mJDistance: 0.7mmStack: 1 | ||
| 4 | 52 | Caucasian, 3 | Genitalia | 3 | 1 | 10 | 3 | 90 | 2 | Fraxis by Creative Ilooda® | Energy: 30–42mJDistance: 0.7mmStack: 1 | ||
| 5 | 49 | Caucasian, 3 | Genitalia | 3 | 1 | 10 | 3 | 80 | 1 | Fraxis by Creative Ilooda® | Energy: 32mJDistance: 0.7mmStack: 1 | ||
| Inframammary | 3 | 0 | 1 | ||||||||||
Abbreviations: Fractional microablative CO2 laser (FMCL) type and parameters applied; IGA: Investigator's Global Assessment; VAS: visual analogue scale.
We included five women. Table 1 illustrates main characteristics of patients and lesions treated. A significant reduction in the IGA score was observed between baseline (3 [2–3]) and after treatment (0 [0–2]) (p=0.01). The median pre-treatment VAS score was 10 (8–10) and the post-treatment VAS score, 3 (0–4), which was significantly lower (p=0.041). The median satisfaction level with the procedure was 90 (80–100). Treatment was well tolerated, and no severe adverse events were reported. Mild and transient erythema, edema and crusting were reported in all the patients. Two patients were sexually active before treatment, experiencing pain with intercourse. They were able to resume painless sexual activity after treatment. No relapses or presence of squamous cell carcinoma were reported in the area at the 36.4-month follow-up (7.2–40.5). Fig. 1 illustrates the results in 1 patient after 1 session of treatment.
, before 2nd laser session (C, right; D, left) and at the 1-year follow-up (E).")
PDT targets inflammatory cells, generating intracellular reactive oxygen species through the interaction of a photosensitizing agent, directed at these cells, and an appropriate light wavelength for agent activation.1 PDT prompts apoptosis in the target tissue, without damaging the surrounding healthy skin.5 PDT has been associated with alleviation of subjective LS symptoms such as pruritus and pain, along with an improvement in patients’ quality of life.5
On the other hand, FMCL induces a superficial ablative effect on the tissue while stimulating the production of collagen and elastic fibers. This process helps restore epithelial trophism and remodel the connective tissue of the dermis.3,4 Recent findings indicate that FMCL provides clinical benefits to as many as 89% of LS patients, a significantly higher proportion vs those using topical corticosteroids.6
The use of a fractionated ablative laser to increase the uptake of topical treatments, termed laser-assisted drug delivery, has already been explored in several skin diseases.7,8 The combination of fractional CO2 laser with PDT has demonstrated greater effectiveness vs PDT alone in conditions such as actinic keratosis9 or basal cell carcinoma.10 Our findings suggest that combining these two techniques could yield synergistic effects also in LS patients arising not only from the distinct skin structures targeted by each technique but also due to FMCL potential to enhance drug permeation, thereby amplifying the effects of PDT.7
There may be concerns on the tolerability of this approach due to pain reported during PDT.5 In our experience, conducted under topical anesthesia, the combination of FMCL plus PDT is a safe and well tolerated procedure.
The main limitations of our study are its retrospective design, the limited number of patients, and the use of two different laser devices. However, we adjusted the settings to create similar laser microchannels.
This is the first case series ever reported to describe the combination of FMCL+PDT to treat refractory LS. This treatment approach seems to be effective in terms of improving disease activity and pain relief, including pain during intercourse, with no associated adverse events, representing a promising alternative for the management of refractory LS.
Ethical approvalReviewed and approved by the “Medicament Research Ethics Committee of the Fundació de Gesció Sanitaria de l’Hospital de la Santa Creu i Sant Pau de Barcelona” (IIBSP-FOT-2023-122).
Informed consentAll patients signed a written informed consent for the publication of data and/or photographs.
FundingNone declared.
Conflicts of interestOY and CM have received transportation assistance from Biofrontera. LM declared no conflicts of interest whatsoever.



