




Tinea capitis is a condition usually found only in children. However, its epidemiological profile has changed in recent decades, with regard to age at onset and the causative microorganisms. We report the cases of 4 women over 65 years of age diagnosed with tinea capitis. One presented plaques of alopecia with desquamation and the other 3 developed crusted inflammatory lesions. Cultures were positive for Trichophyton tonsurans (2 patients), Trichophyton rubrum, and Trichophyton mentagrophytes.
The relative rarity of tinea capitis in the elderly and the frequently atypical presentation in this age group can delay diagnosis, leading to irreversible sequelae and increasing the risk of contagion. Fungal culture should be included in the study of persistent, atypical dermatoses of the scalp, particularly in the elderly.
La tinea capitis se ha considerado clásicamente como un proceso casi exclusivo de la infancia. Sin embargo, en las últimas décadas se han observado algunos cambios en su perfil epidemiológico, tanto en lo que concierne a las edades de presentación como a los agentes responsables.
Se describen los casos de 4 mujeres mayores de 65 años diagnosticadas de tinea capitis. Una de ellas presentaba placas alopécicas con descamación, mientras que en las otras tres las lesiones eran inflamatorias y costrosas. Los cultivos fueron positivos para Trichophyton tonsurans (2 pacientes), Trichophyton rubrum y Trichophyton mentagrophytes.
La relativa infrecuencia de la tinea capitis en la edad avanzada y, por otra parte, su frecuente atipicidad clínica condicionan un diagnóstico tardío, circunstancia que puede condicionar secuelas irreversibles e incrementa la posibilidad de contagios. El cultivo fúngico debería incorporarse en el estudio de las dermatosis del cuero cabelludo de curso atípico y persistente, especialmente en individuos de edad avanzada.
Tinea capitis was thought to be found almost exclusively in children1–4 and most commonly caused by Microsporum audouinii or Microsporum canis.2–7 In recent years, however, the epidemiological profile of the disease has changed in terms of both incidence and causative agents, and its prevalence has increased in adult patients, especially elderly women.3–7 In order to correctly diagnose and manage tinea capitis, physicians need to be familiar with the clinical signs of the disease in elderly patients, as well as the therapeutic responses seen in this age group.
We present 4 cases of tinea capitis in elderly women with atypical clinical manifestations and pathogens (Table 1). All 4 cases were diagnosed in the dermatology department of our hospital in the past 6 months.
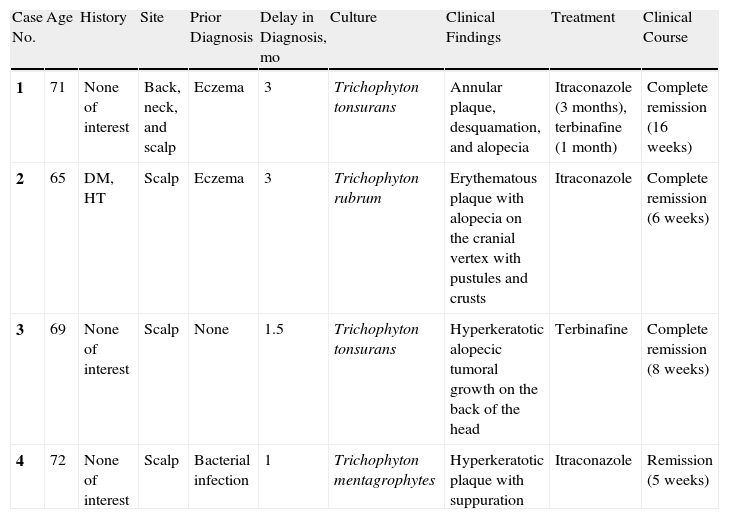
Summary of the 4 clinical cases.
| Case No. | Age | History | Site | Prior Diagnosis | Delay in Diagnosis, mo | Culture | Clinical Findings | Treatment | Clinical Course |
| 1 | 71 | None of interest | Back, neck, and scalp | Eczema | 3 | Trichophyton tonsurans | Annular plaque, desquamation, and alopecia | Itraconazole (3 months), terbinafine (1 month) | Complete remission (16 weeks) |
| 2 | 65 | DM, HT | Scalp | Eczema | 3 | Trichophyton rubrum | Erythematous plaque with alopecia on the cranial vertex with pustules and crusts | Itraconazole | Complete remission (6 weeks) |
| 3 | 69 | None of interest | Scalp | None | 1.5 | Trichophyton tonsurans | Hyperkeratotic alopecic tumoral growth on the back of the head | Terbinafine | Complete remission (8 weeks) |
| 4 | 72 | None of interest | Scalp | Bacterial infection | 1 | Trichophyton mentagrophytes | Hyperkeratotic plaque with suppuration | Itraconazole | Remission (5 weeks) |
DM: diabetes mellitus; HT: hypertension.
The patient was a 71-year-old woman who presented with hair loss and pruritic lesions on her back and scalp. The symptoms had first appeared 3 months earlier. The patient had been diagnosed with eczema and had received treatment with topical corticosteroids for several months. The pruritus had decreased slightly, but the alopecia had progressively worsened. The patient had not been in contact with animals. Physical examination revealed a scaly, erythematous annular plaque covering the neck and the upper third of the back. A large alopecic plaque with abundant whitish desquamation was present on the scalp (Fig. 1), and hair fell out easily with traction. Skin-scale and hair samples were collected for direct microscopic examination using the potassium hydroxide technique, which revealed hyphae, and for culture, which was positive for Trichophyton tonsurans. Oral treatment with itraconazole (200mg/day) resulted in marked improvement in the lesions at 1 month. After that, however, improvement slowed, despite the fact that the patient reported taking the drugs correctly. Clinical symptoms persisted and cultures were still positive 7 months after the start of treatment. The treatment was therefore changed to oral terbinafine (250mg/day), which resulted in complete resolution within 1 month.
Case Description 2
The patient was a 65-year-old woman who presented with slightly pruritic scalp lesions that had appeared 3 months earlier. During the preceding 3 months, she had received treatment with topical corticosteroids, antibiotics, and ciclopirox olamine shampoo, but her condition had not improved. The patient had not been in contact with animals or with people who had similar lesions. Physical examination revealed an erythematous, partially alopecic plaque on the cranial vertex characterized by superficial crusts and pustules (Fig. 2). Histopathologic examination of the biopsy specimen revealed clear evidence of folliculitis and a granulomatous foreign-body reaction. The bacterial culture was negative and Trichophyton rubrum colonies were isolated in the fungal culture. Oral treatment with itraconazole (200mg/day) was initiated and the clinical and microbiologic symptoms resolved completely after 6 weeks.
Case Description 3
The patient was a 69-year-old woman who presented with a crusted tumoral growth on her scalp that had appeared 6 weeks earlier. She had received no prior topical or systemic treatment. Physical examination revealed a crusted lesion on the back of the head. The crust concealed fleshy exophytic granulation tissue. Fungal culture was positive for T tonsurans. Eight weeks after oral treatment with terbinafine (250mg/day) was initiated, there was still some evidence of scarring alopecia but no signs of inflammation, desquamation, or traction hair loss.
Case Description 4The patient was a 72-year-old woman who presented with a 3-week history of 2 crusted, inflammatory lesions on her scalp. She had completed a 3-day treatment with topical corticosteroids and oral cloxacillin. The perilesional erythema had resolved but the rest of the lesion had not improved. The patient had no fever or other symptoms. Physical examination revealed one crusted lesion on the left parietal-temporal region of the scalp (Fig. 3) and another on the forehead. The crust was removed from the lesion on the forehead, revealing an eroded surface with suppuration at various points. Regional lymph nodes were enlarged and palpable.

Although an initial biopsy showed nonspecific changes, a second histologic study revealed the presence of mixed dermal infiltration with numerous eosinophils, as well as spores and filaments inside the follicles. These findings, together with positive culture results, allowed us to establish a diagnosis of Trichophyton mentagrophytes infection. Oral treatment with itraconazole (200mg/day) was initiated. The symptoms improved slowly, resolving completely within 35 days of the start of treatment.
DiscussionThis case series shows that scalp ringworm in elderly patients is relatively common and often presents with atypical clinical characteristics. Low clinical suspicion can lead to inappropriate empiric treatments that delay diagnosis and complicate the therapeutic response.Tinea capitis is usually seen in children between the ages of 3 and 7.1 Although the disease was once thought to be rare in adulthood, a growing number of authors have reported an increase in tinea capitis among adults, particularly menopausal and elderly women.2–6
Factors that may favor the development of the disease at this age include hormonal changes, the use of certain hair-care products, and using the services of hair salons, which can be a source of infection.6,7
In most of the cases that have been reported, including our own case series, diagnosis was delayed.5 This delay is probably due to both the rarity of this infection in adults and its atypical clinical manifestations, which can be confused with inflammatory processes such as seborrheic dermatitis or psoriasis. Atypical manifestations seem to be more common in patients infected with T tonsurans (as in 2 of our cases), who often present either diffuse desquamation with mild alopecia and lesions suggestive of seborrheic dermatitis or pustular inflammatory lesions and associated regional lymphadenopathy, a clinical picture that can lead to an incorrect diagnosis of bacterial infection.4,5,8,9 Although M canis remains the most common causative agent of tinea capitis in southern Europe, with a prevalence greater than 80%,3 the epidemiology of these infections has changed considerably in recent years. A growing number of cases have been attributed to the following species: T mentagrophytes, Trichophyton verrucosum, T tonsurans,3,10,11 and T rubrum.10 Specifically in Barcelona, T mentagrophytes12 has been highly prevalent, whereas T tonsurans is the species most frequently isolated in the United States, the United Kingdom, and Canada.3,13,14
These changes are attributable to many factors, in particular the rise of travel to endemic areas and the migratory flows from the Southern to the Northern hemisphere. In addition to facilitating contagion, migration has also helped to spread species endemic to Africa and Asia–generally anthropophilic fungi–to urban areas in Europe, especially neighborhoods where immigrants make up a high percentage of the population.10,11,14 In keeping with what seems to be the current trend for this disease, the species found in our 4 patients–all city dwellers–were anthropophilic.
It should be noted that fungal culture was essential to either confirming the clinical suspicion or redirecting the diagnosis in all 4 cases. Fungal culture should therefore be used routinely in cases of desquamative conditions of the scalp that involve pruritus or an inflammatory appearance, especially in elderly patients whose symptoms do not respond satisfactorily to the prescribed treatment. It should also be emphasized that patients with fungal infections of the skin are often referred to a specialist–as 3 of the patients in this series were–after receiving treatment with topical corticosteroids, which mask the clinical presentation and further modify the patient's response, or with azole shampoos, which do not resolve the process but can affect the sensitivity of diagnostic tests.
The diversity of the treatments prescribed in this series can be explained by the preferences of the various physicians caring for the different patients. Although griseofulvin remains, for some authors, the treatment of choice for scalp ringworm in children and adults, both terbinafine and itraconazole are considered acceptable alternatives (the latter in particular for cases caused by fungi of the genus Trichophyton).
It should be noted that the disease's apparent resistance to itraconazole–a drug considered effective against tinea capitis–in the case of the first patient may be associated with failure to follow the prescribed regimen strictly. Moreover, in most of the cases in the literature reporting a good response, the dose recommended is 200mg/day, although some authors recommend a dose of 5mg/kg/day. The recommended dose in the first patient in this series would therefore be between 300 and 400mg/day as the patient weighed approximately 65kg. No resistance to itraconazole has been reported in cases of scalp ringworm caused by T tonsurans. Itraconazole resistance has been reported, however, in cases caused by T mentagrophytes (in Latin America), and cases caused by T tonsurans have shown resistance to fluconazole.15–18
In conclusion, the differential diagnosis of any scaly and/or inflammatory skin condition in elderly patients, including those with alopecia, should include tinea capitis, and fungal cultures should be performed routinely in cases of suboptimal response to anti-inflammatory treatments.
Conflict of InterestThe authors have no conflict of interest to declare.
Please cite this article as: Morell L, et al. Tinea capitis en mujeres de edad avanzada: descripción de 4 caso. Actas Dermosifiliogr.2012;103:144-148.



