





Allergic contact dermatitis due to fragrances usually manifests as subacute or chronic dermatitis because fragrances are found in a wide range of products to which patients are repeatedly exposed. The typical patient is a middle-aged woman with dermatitis on her hands and face, although other sites may be affected depending on the allergen and the product in which it is found. The standard patch test series of the Spanish Contact Dermatitis and Skin Allergy Research Group (GEIDAC) contains 4 fragrance markers: balsam of Peru, fragrance mix i, fragrance mix ii, and lyral. Testing with a specific fragrance series is recommended in patients with a positive result to any of these 4 markers. The use of a specific fragrance series and new legislation obliging manufacturers to specify the fragrances used in their products, will help to improve the management of allergic contact dermatitis due to fragrances.
La dermatitis de contacto alérgica por fragancias suele presentarse clínicamente como un eczema subagudo o crónico debido a la ubicuidad de este alérgeno en los productos de uso cotidiano y el contacto repetido. El paciente típico es una mujer de edad media con afectación de las manos y la cara, aunque la localización de las lesiones variará dependiendo del alérgeno y del producto causante. Dentro de la batería estándar del Grupo Español en Investigación de Dermatitis de Contacto y Alergia Cutánea (GEIDAC) están incluidos 4 marcadores de fragancias: el bálsamo del Perú, la mezcla de fragancias i, la mezcla de fragancias ii y el lyral. En caso de que alguno de estos marcadores sea positivo está indicada la utilización de una serie de fragancias específicas para el diagnóstico. Esto, unido a la nueva legislación que obliga a la industria a notificar qué ingredientes y fragancias utiliza en sus productos, nos ayudará a la resolución de la dermatitis de pacientes alérgicos.
The primary objective of this article is to provide an update on the current situation regarding allergic contact dermatitis caused by fragrances. In Part 1, we reviewed relevant legislation, the main sources of exposure, and epidemiology. In Part 2, we focus on the usual clinical manifestations of this disease and propose an algorithm for the diagnosis and treatment of affected patients.
Clinical FeaturesAllergic contact dermatitis is the most common cutaneous adverse effect associated with the use of fragrances.1 It manifests mainly as subacute or chronic eczema caused by contact with fragrance allergens, a group of substances that are difficult to avoid in daily life. The typical patient is a 40-year-old woman with dermatitis affecting the hands or face,2–4 although any part of the body can be affected, depending on the the type of product used and the area it is applied to.5 Most studies find the hands to be the site most commonly affected by cosmetic products1,5–7 and even more so by products used in the household and the workplace.8 Fragrances are seldom the only cause of hand eczema, and their application often complicates underlying conditions, such as irritant dermatitis and atopic dermatitis.9,10 Some series find the face to be the most commonly affected site11 by direct application of cosmetic products, although airborne fragrances can also be responsible. Another frequently affected site is the legs in patients with vascular ulcers who become sensitized to the fragrance ingredients in their topical medication.12,13 A history of axillary eczema associated with deodorant or of cutaneous rash at sites where cologne or perfume is applied significantly increases the likelihood of a patient being allergic to fragrances. Fragrances are considered to be the most common cause of primary sensitization.14
The neck is commonly affected by contact dermatitis due to fragrance allergy (Fig. 1) as a result of the direct application of perfumes and colognes. The presence of eczematous lesions on the laryngeal prominence (Adam's apple) as a result of the application of aerosolized perfume is known as the atomizer sign.15

Cheilitis, which is usually a chronic disease, can be allergic in origin and caused by fragrances. A retrospective study of 129 patients with cheilitis found the second most common cause to be allergens found in cosmetic, dental, and food products.16
Fragrances can cause skin diseases other than allergic contact dermatitis, as follows:
- 1
Contact urticaria may be allergic or nonallergic, and wheals are sometimes associated with respiratory symptoms.17 Cases of contact urticaria have been reported after application of skin patches containing cinnamic aldehyde, cinnamyl alcohol, and balsam of Peru.18
- 2
Irritant contact dermatitis is associated with products containing high concentrations of fragrances, particularly deodorants, because they are applied to moist areas of delicate skin, such as the axilla. Other affected sites include the eyelids and the perineum.19
- 3
Contact dermatitis caused by exposure to the sun after application of fragrances includes photoallergic dermatitis and phototoxic dermatitis. Photoallergic contact dermatitis to fragrances has been reported with coumarin and oakmoss absolute,20–22 but the most common cause is musk ambrette, a compound which was used in various products as a fragrance fixative23 and is now prohibited. Positive photopatch reactions have been reported with oakmoss absolute, eugenol, cinnamic aldehyde, 6-methyl coumarin, and hydroxycitronellal, although most were interpreted as phototoxic reactions.20 Poikiloderma of Civatte, a condition characterized by irregular hyperpigmented plaques with unevenly distributed telangiectases and mild atrophy on the sides of the neck, is the result of chronic actinic damage. Some authors believe it to be a phototoxic reaction associated with the application of fragrance in this area.24,25 Berloque dermatitis is a proven phototoxic reaction26 consisting of brownish-red lesions that arise on the area where a perfume or cologne is applied when the skin is exposed to sunlight.
- 4
Pigmented cosmetic dermatitis, first described in Japan in the 1970s, is the result of contact allergy to the ingredients of cosmetic products, including fragrances.27 The symptoms are similar to those of Riehl melanosis. Positive patch test results have demonstrated a direct association with geraniol, benzyl alcohol, methoxycitronellal, and several essential oils (eg, ylang-ylang and jasmine absolute). Fragrances can also cause depigmentation of the skin.
- 5
Isolated reports have been published of other clinical conditions associated with fragrances, including bullous contact allergy28 and erythema multiforme.29
The information supplied by the patient leads us to suspect fragrance allergy, especially when the area affected is one where a cosmetic product with a high fragrance concentration (eg, cologne, perfume, or deodorant) is commonly applied. The history should include the cosmetic products used by the patient and exacerbating factors such as profession, hobbies, and exposure to sunlight. In the physical examination, the presence of dermatitis on the face, retroauricular area, axilla, chest, or anal/vulvar area should alert the physician to the possibility of fragrance allergy. However, any part of the body can be affected. Furthermore, other forms of dermatitis (irritant, atopic) can be complicated by sensitization to fragrances.
A confirmed diagnosis of allergic contact eczema is based on symptoms and patch testing, the results of which should be clinically relevant.
Allergens Used in Patch TestsOf the more than 2800 substances catalogued as fragrances by the Research Institute of Fragrance Materials, at least 100 are allergenic.30 Fortunately, the fact that only a limited number are responsible for most cases of sensitization facilitates detection of allergy using patch tests in which small groups of fragrances are analyzed together in mixes.
The Spanish Contact Dermatitis and Skin Allergy Research Group (GEIDAC) standard series contains 2 fragrance markers: balsam of Peru and fragrance mix I. At the last meeting of GEIDAC, it was agreed that fragrance mix II and lyral would be included in the standard series from January 1, 2012. Colophony is an oleoresin considered by some authors to be a marker of sensitivity to fragrances.31 Nevertheless, most studies and our daily practice show the limited usefulness of this substance in the diagnosis of sensitivity.32 The same is true of propolis, which is not useful as a marker of allergy to fragrances, although it has been proposed as such by some authors.31 Sesquiterpene lactones are essentially markers of contact allergy to plants, and positive test results in patients with fragrance allergy are thought mainly to be due to cross-reaction.33
Balsam of PeruBalsam of Peru is the most widely used marker for diagnosis of fragrance allergy. This natural resin extracted from Myroxylon pereirae, a tree that grows in Central and South America, was originally used to heal wounds and cure infections.34 In 1974, the use of natural balsam of Peru as a fragrance ingredient was prohibited, and the use of its extracts and distillates in commercial products was restricted to a maximum concentration of 0.4%. Today, we find it in perfumes, cleaning products, topical medications, dental cement and liquids, cosmetic products, and food aroma compounds. Balsam of Peru is composed of 250 chemical substances; the structure of at least 189 is known. Some of these components are fragrance allergens (eg, cinnamyl alcohol, cinnamic aldehyde, eugenol, and isoeugenol).35
In 1948, Bonnevie36 reported that balsam of Peru was a common allergen and identified cinnamic aldehyde as an important allergic ingredient. Hausen37 tested the components of balsam of Peru in 102 patients who had a positive reaction to this marker and found the main culprit allergen to be a fragrance, cinnamyl alcohol. The second fragrance identified, eugenol, was the sixth most common allergen. The role of balsam of Peru as a marker of allergy to fragrances is more complex and heterogeneous than that of fragrance mix I.2 Balsam of Peru obtains a positive result in approximately 50% of cases of fragrance allergy, and has been reported to cross-react with colophony, balsam of Tolu, cinnamates, benzoates, benzylsalicylates, coumarin, farnesol, propolis, and diethylbestrol.35
Fragrance Mix IFragrance mix I, the second mixture used to test for fragrance allergies, was introduced as a marker in the standard series after the publications by Larsen38,39 in the late seventies. It has 8 components, namely, 7 synthetic fragrances and 1 natural fragrance. Initially, each of the fragrances was tested at 2% (total of 16%); however, this approach generated a large number of false-positive results because of irritant action. Therefore, in 1984, the concentration was reduced to 1% (total of 8%).
Table 1 lists important information on the components of fragrance mix I.
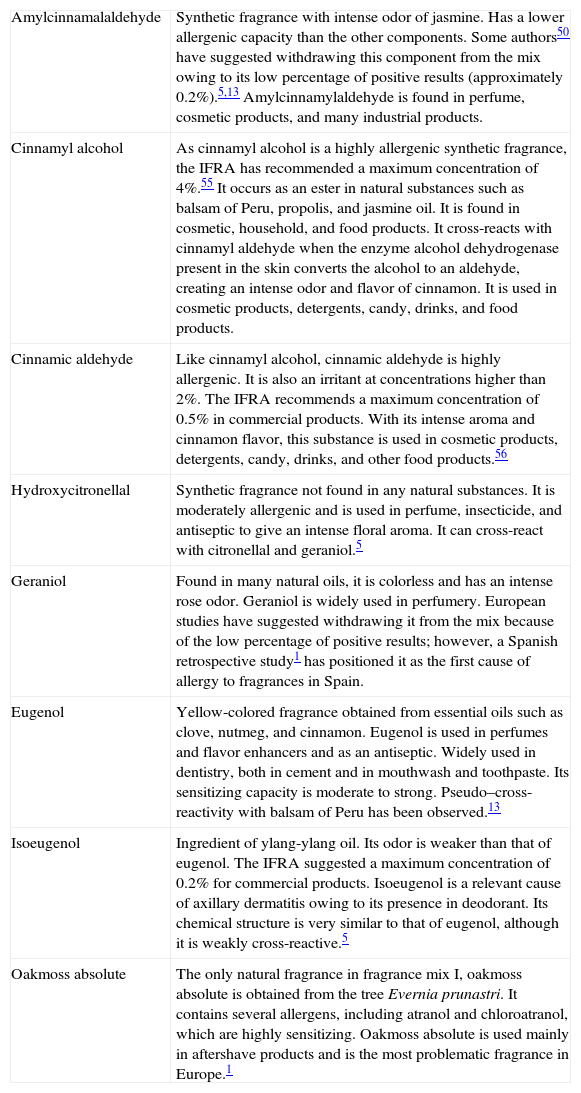
Components of Fragrance Mix I.
| Amylcinnamalaldehyde | Synthetic fragrance with intense odor of jasmine. Has a lower allergenic capacity than the other components. Some authors50 have suggested withdrawing this component from the mix owing to its low percentage of positive results (approximately 0.2%).5,13 Amylcinnamylaldehyde is found in perfume, cosmetic products, and many industrial products. |
| Cinnamyl alcohol | As cinnamyl alcohol is a highly allergenic synthetic fragrance, the IFRA has recommended a maximum concentration of 4%.55 It occurs as an ester in natural substances such as balsam of Peru, propolis, and jasmine oil. It is found in cosmetic, household, and food products. It cross-reacts with cinnamyl aldehyde when the enzyme alcohol dehydrogenase present in the skin converts the alcohol to an aldehyde, creating an intense odor and flavor of cinnamon. It is used in cosmetic products, detergents, candy, drinks, and food products. |
| Cinnamic aldehyde | Like cinnamyl alcohol, cinnamic aldehyde is highly allergenic. It is also an irritant at concentrations higher than 2%. The IFRA recommends a maximum concentration of 0.5% in commercial products. With its intense aroma and cinnamon flavor, this substance is used in cosmetic products, detergents, candy, drinks, and other food products.56 |
| Hydroxycitronellal | Synthetic fragrance not found in any natural substances. It is moderately allergenic and is used in perfume, insecticide, and antiseptic to give an intense floral aroma. It can cross-react with citronellal and geraniol.5 |
| Geraniol | Found in many natural oils, it is colorless and has an intense rose odor. Geraniol is widely used in perfumery. European studies have suggested withdrawing it from the mix because of the low percentage of positive results; however, a Spanish retrospective study1 has positioned it as the first cause of allergy to fragrances in Spain. |
| Eugenol | Yellow-colored fragrance obtained from essential oils such as clove, nutmeg, and cinnamon. Eugenol is used in perfumes and flavor enhancers and as an antiseptic. Widely used in dentistry, both in cement and in mouthwash and toothpaste. Its sensitizing capacity is moderate to strong. Pseudo–cross-reactivity with balsam of Peru has been observed.13 |
| Isoeugenol | Ingredient of ylang-ylang oil. Its odor is weaker than that of eugenol. The IFRA suggested a maximum concentration of 0.2% for commercial products. Isoeugenol is a relevant cause of axillary dermatitis owing to its presence in deodorant. Its chemical structure is very similar to that of eugenol, although it is weakly cross-reactive.5 |
| Oakmoss absolute | The only natural fragrance in fragrance mix I, oakmoss absolute is obtained from the tree Evernia prunastri. It contains several allergens, including atranol and chloroatranol, which are highly sensitizing. Oakmoss absolute is used mainly in aftershave products and is the most problematic fragrance in Europe.1 |
Abbreviation: IFRA, International Fragrance Association.
In some of the series marketed, sorbitan sesquioleate 5% is used as an emulsifier in both balsam of Peru and fragrance mix I. Enders et al40 demonstrated that sorbitan sesquioleate improved the diagnostic value of these markers because it acts as a vehicle for the fragrances. The only disadvantage of this emulsifier is its occasional allergenic capacity. Consequently, some authors recommend including sorbitan sesquioleate in the specific fragrance series1,2,9 to rule it out as an allergen. In patients who have a positive reaction to both balsam of Peru and fragrance mix I, up to 17.7% of reactions are false-positive and the patients are in fact allergic to the emulsifier.1
The clinical relevance of these markers varies according to the series, with values ranging from 79% to 92.8% for fragrance mix I and from 66% to 85.71% for balsam of Peru in studies from Spanish hospital centers.1,41 These figures are very high if we compare them with those reported in other international series. We believe this is mainly because the authors who obtain the highest clinical relevance are those who consider fragrance allergy an exacerbating factor in patients with other underlying skin diseases (eg, atopic or irritant dermatitis) when patch testing is positive for fragrances.
Recent studies showed that the 2 fragrance markers in the current GEIDAC standard series—balsam of Peru and fragrance mix I—continue to be efficacious and detect between 70% and 90% of fragrance-allergic patients.1,2,42 Some authors have even identified fragrance allergy in up to 85% of patients using only fragrance mix I. Nevertheless, in the last few years, new fragrance markers have been developed that reflect advances in the industry, which brings products with new fragrances onto the market. Recent findings show that around 15% of fragrance-allergic patients are not detected by these 2 markers.43 Since 2005, experts have been studying the use of fragrance mix II and hydroxyisohexyl 3-cyclohexane carboxaldehyde (lyral) as markers of sensitization to fragrance in some standard series in Europe.
Fragrance Mix IIIn 2005, Frosch et al.44,45 studied a new tool—fragrance mix II—with the aim of detecting a greater number of patients sensitized to fragrances, including those not diagnosed after application of the usual markers. Fragrance mix II is composed of 6 fragrances at different concentrations (Table 2). In 2005, this mix was included in the series of the German contact allergy group (Deutschen Kontaktallergie-Gruppe), and since 2008, it has formed part of the European standard series.46 In 2010, data collected by the Informationverbund Dermatologischer Kliniken were published on patients tested with this mix in several European centers between 2005 and 2008.47 Of the 35 633 patients included, 4.9% had positive results with fragrance mix II; the most common allergens detected with this series, in decreasing order of frequency, were as follows: lyral (in almost half of the sample), citral, farnesol, hexylcinnamal, coumarin, and citronellol.
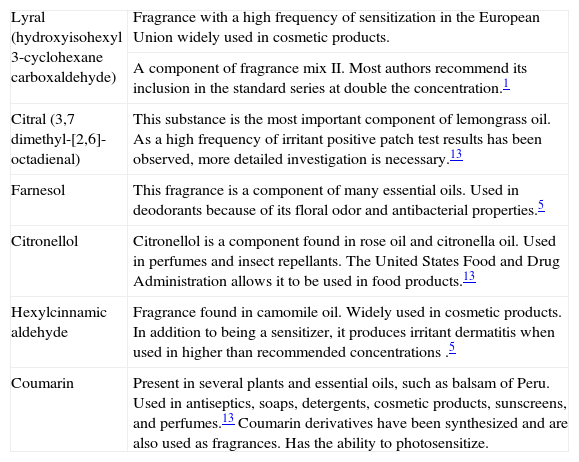
Components of Fragrance Mix II (Standard Series of the Spanish Contact Dermatitis and Skin Allergy Research Group).
| Lyral (hydroxyisohexyl 3-cyclohexane carboxaldehyde) | Fragrance with a high frequency of sensitization in the European Union widely used in cosmetic products. |
| A component of fragrance mix II. Most authors recommend its inclusion in the standard series at double the concentration.1 | |
| Citral (3,7 dimethyl-[2,6]-octadienal) | This substance is the most important component of lemongrass oil. As a high frequency of irritant positive patch test results has been observed, more detailed investigation is necessary.13 |
| Farnesol | This fragrance is a component of many essential oils. Used in deodorants because of its floral odor and antibacterial properties.5 |
| Citronellol | Citronellol is a component found in rose oil and citronella oil. Used in perfumes and insect repellants. The United States Food and Drug Administration allows it to be used in food products.13 |
| Hexylcinnamic aldehyde | Fragrance found in camomile oil. Widely used in cosmetic products. In addition to being a sensitizer, it produces irritant dermatitis when used in higher than recommended concentrations .5 |
| Coumarin | Present in several plants and essential oils, such as balsam of Peru. Used in antiseptics, soaps, detergents, cosmetic products, sunscreens, and perfumes.13 Coumarin derivatives have been synthesized and are also used as fragrances. Has the ability to photosensitize. |
Most studies analyzing the usefulness of this mix agree with the recommendation that it should be included in the standard series, since it detects a considerable number of fragrance-allergic patients who would not be diagnosed by fragrance mix I and balsam of Peru. Negative reactions to fragrance mix I have been recorded in 32% of patients with a positive reaction to fragrance mix II.44 Some European countries have already included this mix in their standard series, and GEIDAC recommended its inclusion in the Spanish standard series as of January 1, 2012 (Fig. 2).
Hydroxyisohexyl 3-Cyclohexane Carboxaldehyde
Hydroxyisohexyl 3-cyclohexane carboxaldehyde (lyral) is included in fragrance mix II at a concentration of 2.5%; however, most authors recommend its inclusion in the standard series at double this concentration (5%). The frequency of sensitization is 1% to 3.1%, and it is often detected in patients with hand eczema.46
When 1 or 2 fragrance markers in the standard series (fragrance mix I, balsam of Peru, or both) are positive, the specific fragrance series should be applied, although the yield is poorer when a positive result is obtained only for balsam of Peru, since in 75% of these cases we will not obtain a positive result for a specific fragrance.
Specific Fragrance SeriesThe number of individual fragrance ingredients tested and the proportions used vary depending on the country and laboratory. The specific series from Martí Tor and Trolab contains each fragrance at 1%. Chemotechnique Diagnostics, however, have doubled the concentration to 2%. This increase has made it possible to detect a larger number of allergic patients, who would have gone undiagnosed with the lower concentration, but it also increases the number of false positives due to irritant reactions.
We believe that the specific series should include all the fragrances in fragrance mixes I and II individually. It should also include the 26 fragrances that must be specified on product labels, since a positive result for any of these substances would allow us to advise the patient to avoid only the specific fragrance(s). Sorbitan sesquioleate should be tested individually as part of this specific series, since it enables us to detect false positives in patients with a positive reaction to either of the mixes caused by allergy to the emulsifier rather than to the fragrance. Other authors9 recommend including this emulsifier in each of the fragrances to increase the diagnostic yield of the series and avoid false negatives.
Products Used by the PatientWe can complete the allergy workup by by testing the patients’ reaction to the products they use, especially if those products are suspected of causing dermatitis. Depending on the product, we can apply it as a patch test or a repeat open application test. The latter method is recommended in the case of highly irritant products, such as colognes or perfumes. In the case of products whose daily application involves removal or rinsing from the skin (eg, shampoos and shower gels), the undiluted product should not be used in patch tests or use tests. The concentration should be reduced to 1% aq or the repeat open application test method should be used, since these approaches can confirm the clinical relevance of the results in some cases.
Emerging FragrancesLinalool (dimethyl octadienol) is a natural fragrance present in many essential oils that has very low sensitizing potential as a pure substance. In recent years, there has been growing awareness that the products of its oxidation are much more allergenic than the fresh or initial chemical substance.35 Matura et al.48 found positive results to linalool in 1.3% of 1511 consecutive patients.49
Trimethyl-benzenepropanolol (majantol) is another fragrance that is not included in the standard mixes or series; however, several studies50 have shown that 0.5% of consecutive patch test patients are sensitized to this ingredient. Larsen et al.51 recommend including majantol in the specific fragrance series.
Patch Test ReadingsThe 2 markers of fragrance allergy currently included in the standard GEIDAC battery are fragrance mix I and balsam of Peru. If a positive reaction is observed to 1 or both of these, the specific fragrance series should be tested. According to De Groot and Frosch,9 if the reaction is weakly positive, the probability of it being irritant is high; therefore, the authors recommend reapplying the marker in a patch test before applying the specific series.
Studies show that no positive reactions are detected with the specific series in 25% to 60% of patients who react to fragrance mix I. There are several possible explanations for this finding. First, the positive response to the mix could be irritant, that is, a false positive. Second, the result may be a false negative to the specific series, because the concentration of the individual fragrances is too low or because the fragrances do not contain the emulsifier sorbitan sesquioleate, which enhances absorption of these substances and is included in the mixes of the standard series. Third, the allergen a patient reacts to could be a combination of several fragrances and not only an individual fragrance, or a synergistic effect could occur when several fragrances are combined.1,2,9
If we obtain positive results for both fragrance mix 1 and balsam of Peru in the standard series, it is more likely that the allergy is actually to fragrances; nevertheless, it is important to rule out sensitization to sorbitan sesquioleate (Fig. 3), the emulsifier that is added to these markers in some series; this can be done by testing it separately in the specific fragrance series.1

Patient with positive test results for fragrance mix I and balsam of Peru. In this case, the results were false-positive, since the patient was sensitized to sorbitan sesquioleate in a topical treatment. This substance is added as an emulsifier to some fragrance mix I and balsam of Peru patches.
Only 25% of patients who have a positive result for balsam of Peru will show a positive result when tested with the specific series.1 Despite the poorer yield, we feel that this approach is worthwhile, since one-quarter of these patients will only have to avoid 1 fragrance rather than stop using all of them.
If both fragrance mix I and II are positive at hospitals that use them as part of their standard series, we should consider cosensitization to geraniol and citral,52 which could be confirmed by applying the specific series.
In the hypothetical case where the clinical suspicion of contact allergy to fragrances is high despite negative patch test results, we must test the specific fragrance series because in more than 9% of cases we will obtain a positive result to at least 1 fragrance and, therefore, a diagnosis.1
Figure 4 shows our proposed diagnostic algorithm.
Treatment
Treatment of fragrance-allergic patients has proven problematic because of the ubiquitous nature of these substances and, until recently, the secrecy surrounding the ingredients of marketed products; therefore, a diagnosis of fragrance allergy used to involve restricting any product containing fragrances.
Since the implementation of the European law regulating mandatory specification of some of the more common fragrances in household and domestic products,53 treatment has changed radically, although certain limitations remain.
Several scenarios can be envisaged, depending on the results of patch tests. If a positive result for 1 of the fragrance markers is followed by 1 or more positive results in the specific fragrance series, we can advise the patient to avoid only those ingredients and use products containing other fragrances.
In 75% of cases with a positive result for balsam of Peru and in 10% to 40% of patients who had positive results for fragrance mix I, we found no definite culprit allergen after testing with the specific fragrance series. In this case, if the markers yield positive results after repeat testing, patients with reactions to balsam of Peru should use only fragrance-free cosmetic, household, and occupational products. Patients allergic to balsam of Peru who experience severe and extensive skin disease could benefit from a diet free of spices such as cinnamon and clove, as well as curry mixes.35
Table 3 sets out our recommendations for fragrance-allergic patients.
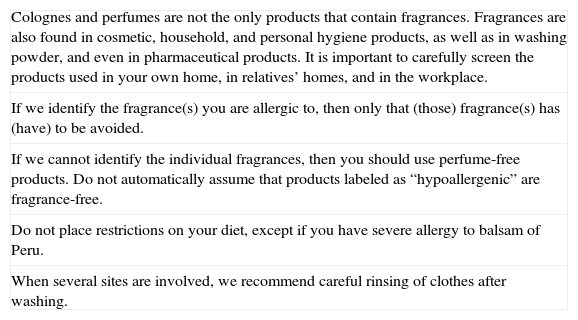
Recommendations for Patients With Fragrance Allergy.
| Colognes and perfumes are not the only products that contain fragrances. Fragrances are also found in cosmetic, household, and personal hygiene products, as well as in washing powder, and even in pharmaceutical products. It is important to carefully screen the products used in your own home, in relatives’ homes, and in the workplace. |
| If we identify the fragrance(s) you are allergic to, then only that (those) fragrance(s) has (have) to be avoided. |
| If we cannot identify the individual fragrances, then you should use perfume-free products. Do not automatically assume that products labeled as “hypoallergenic” are fragrance-free. |
| Do not place restrictions on your diet, except if you have severe allergy to balsam of Peru. |
| When several sites are involved, we recommend careful rinsing of clothes after washing. |
Primary preventive measures that can be applied before contact sensitization occurs include regulation of the maximum permissible concentration of fragrances in commercial products and the creation of new synthetic substances with less allergenic potential than the original products. One example of such a product is oakmoss absolute, a fragrance ingredient from which the main allergens—atranol and chloroatronol—have been eliminated.54
Individual Secondary PreventionRecommendations on secondary prevention have been provided elsewhere in the text (see above).
ConclusionContact dermatitis due to fragrance allergy is common. The markers included in the current Spanish standard series for detection of fragrance allergy (fragrance mix I and balsam of Peru) are good, but there is room for improvement. In recent years, new markers—fragrance mix II and lyral—have been developed and included in the series of other countries; these markers have proven useful for detecting fragrance-allergic patients who previously went undiagnosed. In our opinion, the specific fragrance series should be applied when the patient tests positive to a fragrance marker, since in most cases specific testing will identify 1 or more fragrances that are—at least in part—responsible for the patient's skin disease. Identifying the specific fragrance allergen has become even more important since the implementation of the law requiring 26 fragrance ingredients to be specified on the labels of commercial products. Before this legislation was enacted, patients diagnosed with fragrance-induced allergic dermatitis faced considerable restrictions on their lifestyle, and the allergy represented a therapeutic challenge for the dermatologist.
Conflict of InterestsThe authors declare that they have no conflicts of interest.
Please cite this article as: Arribas MP, et al. Dermatitis de contacto alérgica por fragancias. Parte II. Actas Dermosifiliogr. 2013;104:29-37.



