






Tattooing has become a popular practice in western countries, particularly among younger populations. Tattoos, however, can cause complications, such as infections, allergic or foreign-body reactions, and even systemic inflammatory responses.
Patients and methodsWe conducted a retrospective study of all patients seen for tattoo-related complications at our skin allergy unit between January 2002 and December 2016.
ResultsWe studied 23 patients. Nine of these experienced early complications, all related to infection. The other 14 patients developed late reactions. Ten were diagnosed with probable allergic contact dermatitis to ink, but the suspect allergen was identified in just 3 cases and confirmed in just 1 of these. There were 2 cases of cutaneous sarcoidosis, 1 case of foreign body granuloma, and 1 case of neuropathy.
ConclusionsComplications resulting from tattoos are relatively common dermatology complaints. Drawing from our experience, we propose a diagnostic algorithm designed to guide dermatologists in evaluating different reactions to tattoos and prescribing appropriate treatment.
Los tatuajes se han convertido en una práctica muy popular en los países occidentales, sobre todo entre los más jóvenes. Las complicaciones asociadas a esta técnica incluyen procesos infecciosos, alérgicos, reacciones a cuerpo extraño e incluso procesos inflamatorios sistémicos.
Pacientes y métodosSe ha realizado un estudio retrospectivo de todos los pacientes que acudieron a la consulta de Alergia cutánea por manifestar complicaciones en un tatuaje desde enero de 2002 a diciembre de 2016.
ResultadosSe han incluido a 23 pacientes. De ellos, 9 presentaron complicaciones de forma precoz y en todos ellos la etiología fue infecciosa. De los 14 pacientes con reacciones tardías, 10 fueron diagnosticados de probable dermatitis de contacto alérgica a la tinta, sin embargo solo en 3 de los casos se pudo apuntar al alérgeno probablemente culpable y tan solo en uno de ellos se pudo demostrar. Se detectaron dos casos de sarcoidosis cutánea, uno de reacción granulomatosa a cuerpo extraño, y un caso de reacción neuropática en una paciente.
ConclusionesLas complicaciones asociadas a los tatuajes son un motivo de consulta relativamente frecuente en las consultas de Dermatología. Proponemos un algoritmo diagnóstico basado en nuestra casuística, que ayude a orientar las distintas reacciones a tatuaje y con ello a iniciar las medidas terapéuticas oportunas.
Tattooing has been used to decorate the skin for different purposes since thousands of years ago. It is a very common practice in many cultures, and its popularity has increased in western countries. The number of reports of associated complications has increased in parallel, and recent publications indicate that the incidence of adverse reactions to permanent tattoos is approximately 2%.1–3 The reactions include infections, acute and chronic inflammatory reactions, and flare-ups of skin complaints due to the isomorphic response. Benign and malignant tumors have also been reported on tattoos, although no causal relationship between the 2 phenomena has been established.4,5 Current Spanish legislation adopts the resolution of the Council of Europe ResAP (2008) on permanent tattoos, which establishes regulations stating that the packaging must show the conditions of use, date of minimum durability, batch number, and the list of ingredients (the Chemical Abstract Service or Color Index number, according to international nomenclature) and guarantee that the content is sterile. However, since most inks used in Spain are imported from Asia and the United States, they are not subject to this regulation.6
The objective of the present study was to describe the clinical characteristics of patients seen at a skin allergy clinic with a tattoo-related complication between January 2002 and December 2016. We also propose an algorithm for managing patients with a suspected allergic reaction to ink and discuss the yield of patch tests and the usefulness of patch testing with the ink itself.
Material and MethodsWe performed a descriptive, retrospective study of all patients who were seen at the Skin Allergy Clinic of Hospital General Universitario de Alicante, Alicante, Spain with a tattoo-related complication. We excluded patients whose reaction was to a temporary tattoo. We recorded epidemiological and clinical variables, as well as the results of additional tests. We divided the cohort into 2 groups: patients who experienced early reactions (within the first month after the tattoo) (Table 1) and patients who experienced late reactions (more than 1 month after the tattoo) (Table 2). In addition, patients were grouped according to the clinical pattern observed based on the classification by Serup et al.5 Patients with a suspected allergic reaction to ink underwent patch testing, which was performed with the standard series of the Grupo Español de Investigación en Dermatitis de Contacto y Alergia Cutánea (Spanish Contact Dermatitis and Skin Allergy Research Group) or a specific textile series (Chemotechnique Diagnostics); in some cases, a specific metal series (Martí Tor) and the ink supplied by the patient were also used (Table 3).
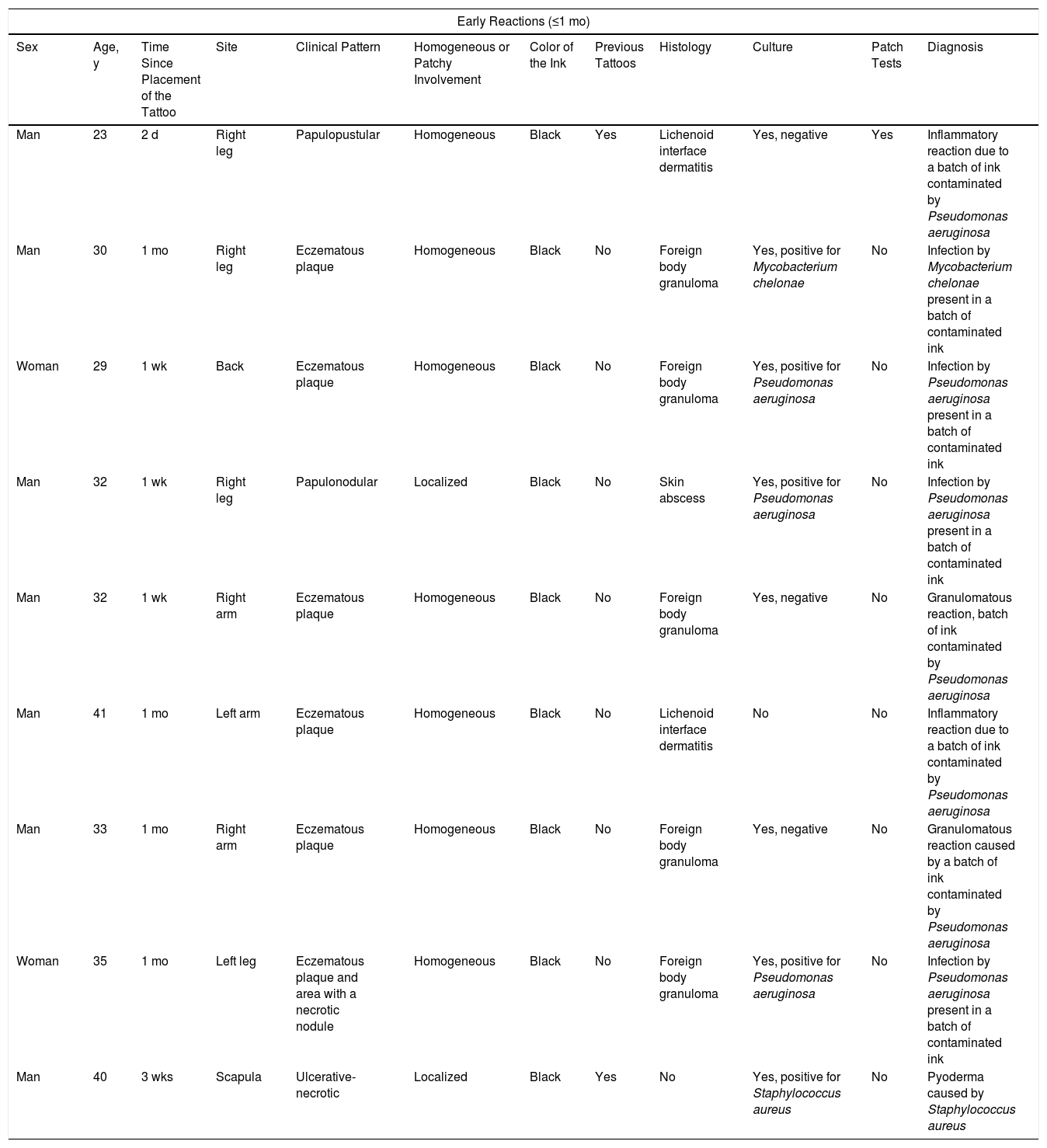
Epidemiological and Clinical Characteristics of Patients Who Experienced Early Reactions: Additional Tests and Final Diagnosis.
| Early Reactions (≤1 mo) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Age, y | Time Since Placement of the Tattoo | Site | Clinical Pattern | Homogeneous or Patchy Involvement | Color of the Ink | Previous Tattoos | Histology | Culture | Patch Tests | Diagnosis |
| Man | 23 | 2 d | Right leg | Papulopustular | Homogeneous | Black | Yes | Lichenoid interface dermatitis | Yes, negative | Yes | Inflammatory reaction due to a batch of ink contaminated by Pseudomonas aeruginosa |
| Man | 30 | 1 mo | Right leg | Eczematous plaque | Homogeneous | Black | No | Foreign body granuloma | Yes, positive for Mycobacterium chelonae | No | Infection by Mycobacterium chelonae present in a batch of contaminated ink |
| Woman | 29 | 1 wk | Back | Eczematous plaque | Homogeneous | Black | No | Foreign body granuloma | Yes, positive for Pseudomonas aeruginosa | No | Infection by Pseudomonas aeruginosa present in a batch of contaminated ink |
| Man | 32 | 1 wk | Right leg | Papulonodular | Localized | Black | No | Skin abscess | Yes, positive for Pseudomonas aeruginosa | No | Infection by Pseudomonas aeruginosa present in a batch of contaminated ink |
| Man | 32 | 1 wk | Right arm | Eczematous plaque | Homogeneous | Black | No | Foreign body granuloma | Yes, negative | No | Granulomatous reaction, batch of ink contaminated by Pseudomonas aeruginosa |
| Man | 41 | 1 mo | Left arm | Eczematous plaque | Homogeneous | Black | No | Lichenoid interface dermatitis | No | No | Inflammatory reaction due to a batch of ink contaminated by Pseudomonas aeruginosa |
| Man | 33 | 1 mo | Right arm | Eczematous plaque | Homogeneous | Black | No | Foreign body granuloma | Yes, negative | No | Granulomatous reaction caused by a batch of ink contaminated by Pseudomonas aeruginosa |
| Woman | 35 | 1 mo | Left leg | Eczematous plaque and area with a necrotic nodule | Homogeneous | Black | No | Foreign body granuloma | Yes, positive for Pseudomonas aeruginosa | No | Infection by Pseudomonas aeruginosa present in a batch of contaminated ink |
| Man | 40 | 3 wks | Scapula | Ulcerative-necrotic | Localized | Black | Yes | No | Yes, positive for Staphylococcus aureus | No | Pyoderma caused by Staphylococcus aureus |
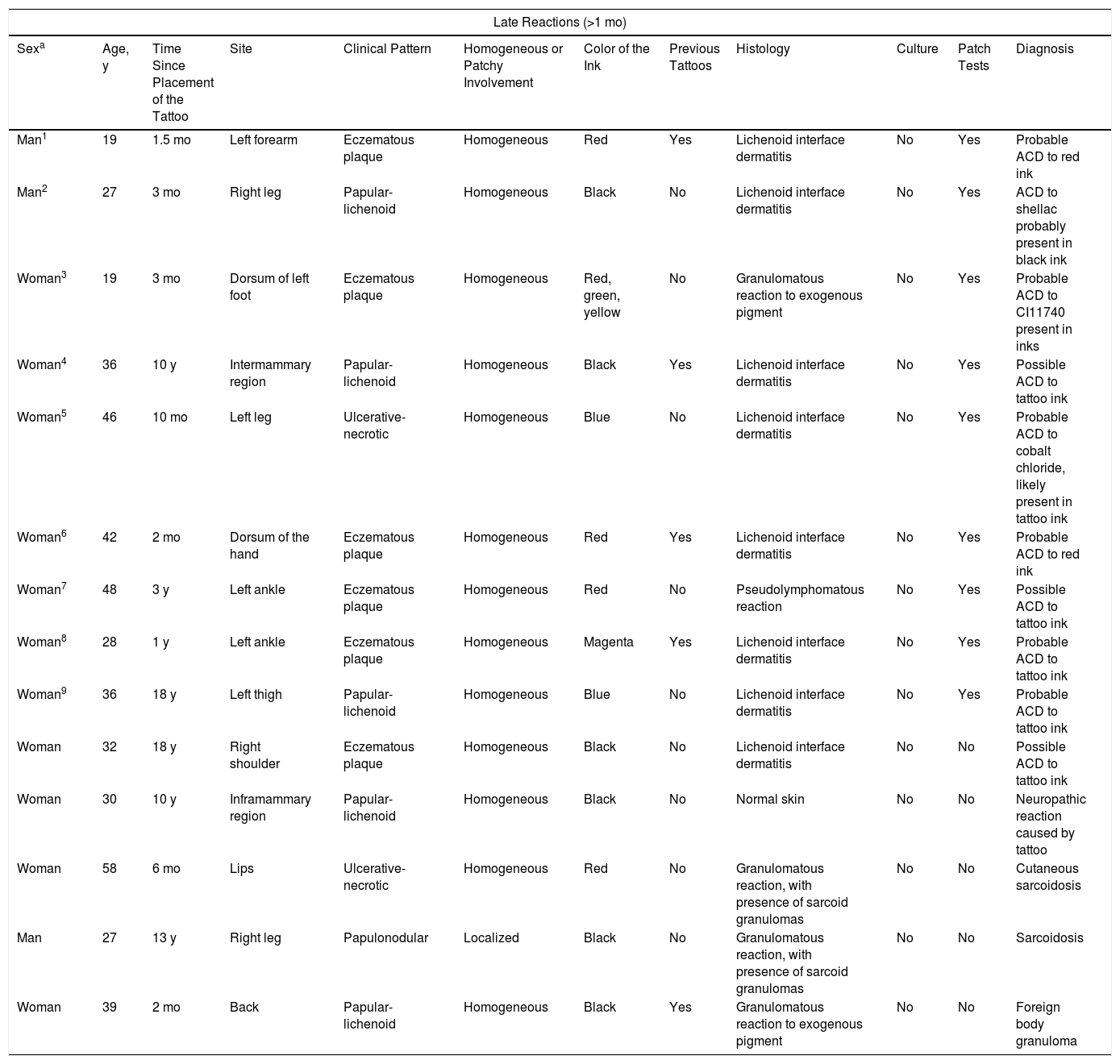
Epidemiological and Clinical Characteristics of Patients Who Experienced Late Reactions.
| Late Reactions (>1 mo) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sexa | Age, y | Time Since Placement of the Tattoo | Site | Clinical Pattern | Homogeneous or Patchy Involvement | Color of the Ink | Previous Tattoos | Histology | Culture | Patch Tests | Diagnosis |
| Man1 | 19 | 1.5 mo | Left forearm | Eczematous plaque | Homogeneous | Red | Yes | Lichenoid interface dermatitis | No | Yes | Probable ACD to red ink |
| Man2 | 27 | 3 mo | Right leg | Papular-lichenoid | Homogeneous | Black | No | Lichenoid interface dermatitis | No | Yes | ACD to shellac probably present in black ink |
| Woman3 | 19 | 3 mo | Dorsum of left foot | Eczematous plaque | Homogeneous | Red, green, yellow | No | Granulomatous reaction to exogenous pigment | No | Yes | Probable ACD to CI11740 present in inks |
| Woman4 | 36 | 10 y | Intermammary region | Papular-lichenoid | Homogeneous | Black | Yes | Lichenoid interface dermatitis | No | Yes | Possible ACD to tattoo ink |
| Woman5 | 46 | 10 mo | Left leg | Ulcerative-necrotic | Homogeneous | Blue | No | Lichenoid interface dermatitis | No | Yes | Probable ACD to cobalt chloride, likely present in tattoo ink |
| Woman6 | 42 | 2 mo | Dorsum of the hand | Eczematous plaque | Homogeneous | Red | Yes | Lichenoid interface dermatitis | No | Yes | Probable ACD to red ink |
| Woman7 | 48 | 3 y | Left ankle | Eczematous plaque | Homogeneous | Red | No | Pseudolymphomatous reaction | No | Yes | Possible ACD to tattoo ink |
| Woman8 | 28 | 1 y | Left ankle | Eczematous plaque | Homogeneous | Magenta | Yes | Lichenoid interface dermatitis | No | Yes | Probable ACD to tattoo ink |
| Woman9 | 36 | 18 y | Left thigh | Papular-lichenoid | Homogeneous | Blue | No | Lichenoid interface dermatitis | No | Yes | Probable ACD to tattoo ink |
| Woman | 32 | 18 y | Right shoulder | Eczematous plaque | Homogeneous | Black | No | Lichenoid interface dermatitis | No | No | Possible ACD to tattoo ink |
| Woman | 30 | 10 y | Inframammary region | Papular-lichenoid | Homogeneous | Black | No | Normal skin | No | No | Neuropathic reaction caused by tattoo |
| Woman | 58 | 6 mo | Lips | Ulcerative-necrotic | Homogeneous | Red | No | Granulomatous reaction, with presence of sarcoid granulomas | No | No | Cutaneous sarcoidosis |
| Man | 27 | 13 y | Right leg | Papulonodular | Localized | Black | No | Granulomatous reaction, with presence of sarcoid granulomas | No | No | Sarcoidosis |
| Woman | 39 | 2 mo | Back | Papular-lichenoid | Homogeneous | Black | Yes | Granulomatous reaction to exogenous pigment | No | No | Foreign body granuloma |
Abbreviation: ACD, allergic contact dermatitis.
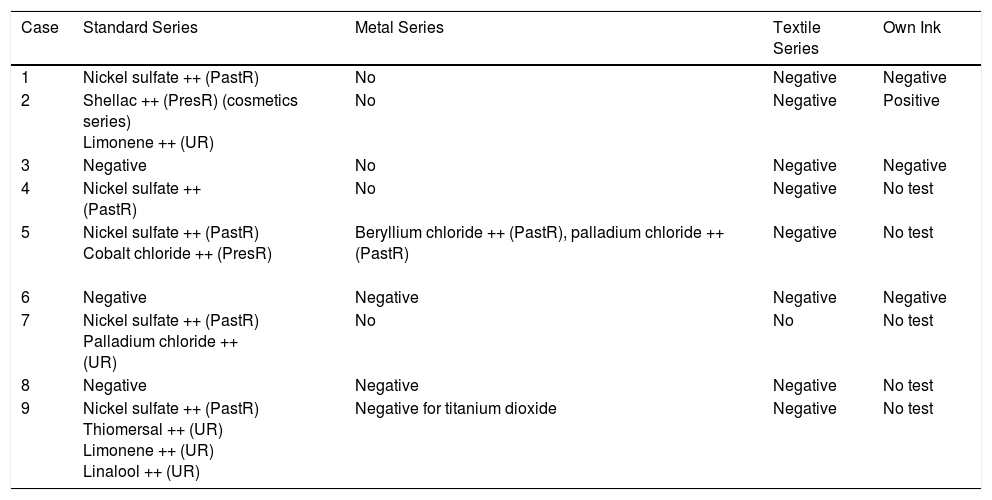
Results of Patch Tests.
| Case | Standard Series | Metal Series | Textile Series | Own Ink |
|---|---|---|---|---|
| 1 | Nickel sulfate ++ (PastR) | No | Negative | Negative |
| 2 | Shellac ++ (PresR) (cosmetics series) Limonene ++ (UR) | No | Negative | Positive |
| 3 | Negative | No | Negative | Negative |
| 4 | Nickel sulfate ++ (PastR) | No | Negative | No test |
| 5 | Nickel sulfate ++ (PastR) Cobalt chloride ++ (PresR) | Beryllium chloride ++ (PastR), palladium chloride ++ (PastR) | Negative | No test |
| 6 | Negative | Negative | Negative | Negative |
| 7 | Nickel sulfate ++ (PastR) Palladium chloride ++ (UR) | No | No | No test |
| 8 | Negative | Negative | Negative | No test |
| 9 | Nickel sulfate ++ (PastR) Thiomersal ++ (UR) Limonene ++ (UR) Linalool ++ (UR) | Negative for titanium dioxide | Negative | No test |
Abbreviations: PastR past relevance; PresR present relevance; UR unknown relevance.
A total of 23 patients consulted for a tattoo-related skin problem from January 2002 to December 2016. Men accounted for 43.5% (n=10) and women for 56.5% (n=13). The mean age was 36 years (range, 19-58 years). Of the 7 patients who had previous tattoos (28%), only 1 had simultaneous complications on the oldest tattoo (Fig. 1).
 Simultaneous reaction on a red tattoo placed 2 years earlier.")
Onset of symptoms was within the first month of having the tattoo in 9 patients (39%), in whom the initial suspicion was infection. Between November 2004 and April 2005, we saw 8 patients who had been tattooed with black ink during the month before the visit by the same tattooist. Subsequent culture of samples from 7 of these patients revealed Pseudomonas aeruginosa in 3 cases. We therefore performed an exhaustive epidemiological study, which revealed a cutaneous inflammatory reaction to the tattoo owing to a batch of black ink that was contaminated by P aeruginosa. One of the patients tattooed with the contaminated ink was coinfected with Mycobacterium chelonae, which was isolated in culture. The remaining patient was diagnosed with pyodermatitis caused by Staphylococcus aureus, with isolation of the microorganism in culture and compatible symptoms. In our study, early reactions on tattoos were caused by infection. All 8 patients underwent skin biopsy, which revealed the most common histologic pattern to be foreign body granuloma.
We included 14 patients with late reactions. Red ink was the problem color in 6 cases (42.85%), black ink in 5 (35.7%), and blue ink in 2 (14.2%). Only 1 patient experienced a reaction affecting 3 colors simultaneously (yellow, green, and red). The 3 inks shared the pigment CI11740 (pigment yellow 65: 4-methoxy-2-nitrophenyl-N-2-methoxyphenyl-3-oxo-butyramide), which could be the culprit substance (Fig. 2).

Of the clinical patterns observed in reactions to a tattoo proposed by Serup et al.,5 the most prevalent in our series were eczematous plaque (n=6, 42.8%) and a lichenoid-papular pattern (n=4, 28.5%), which were finally associated with a probable diagnosis of allergic contact dermatitis to the ink. An ulcerative-necrotic pattern was observed in 2 patients (14.28%), who had been diagnosed with allergic contact dermatitis to ink in one case and cutaneous sarcoidosis in the other. One patient presented a papulonodular pattern that affected a specific area of the tattoo but spared the remainder of the tattooed skin and was diagnosed as cutaneous sarcoidosis (Fig. 3). Another patient complained of pruritus and dysesthesia on a tattoo in black ink that had been placed 10 years previously; we interpret this finding as a neuropathic pattern, since the biopsy revealed no pathologic findings. Skin biopsies were performed in all cases. In the 10 patients with a probable allergic reaction to the ink color, histopathology revealed lichenoid interface dermatitis in 8 cases (80%). As for the remaining 20%, we observed a pseudolymphomatous pattern in one case and foreign body granuloma in the other. Biopsy confirmed the diagnosis of cutaneous sarcoidosis in 2 of the late-onset cases.

Patch testing was performed in 9 patients whose clinical and histopathologic data were compatible with allergic contact dermatitis to tattoo ink. The standard series was applied, and in some cases the specific textile series and the specific metal series were also applied. Nickel sulphate was the most frequently positive substance (n=4, 44.4%), and its relevance was past in all cases. One patient tested positive for cobalt chloride (++), palladium chloride (++), and beryllium chloride (++). Given that the culprit ink was blue, relevance was thought to be probable for the cobalt chloride patch and unknown for the remaining positive patches. The metal series was used in 4 cases (44.4%), and the results were negative with unknown relevance. The specific textile series was applied in 8 patients (88%), and the results were negative in all cases. In 4 patients (44.4%), patch testing with the ink brought by the patient yielded a positive result in only 1 case.
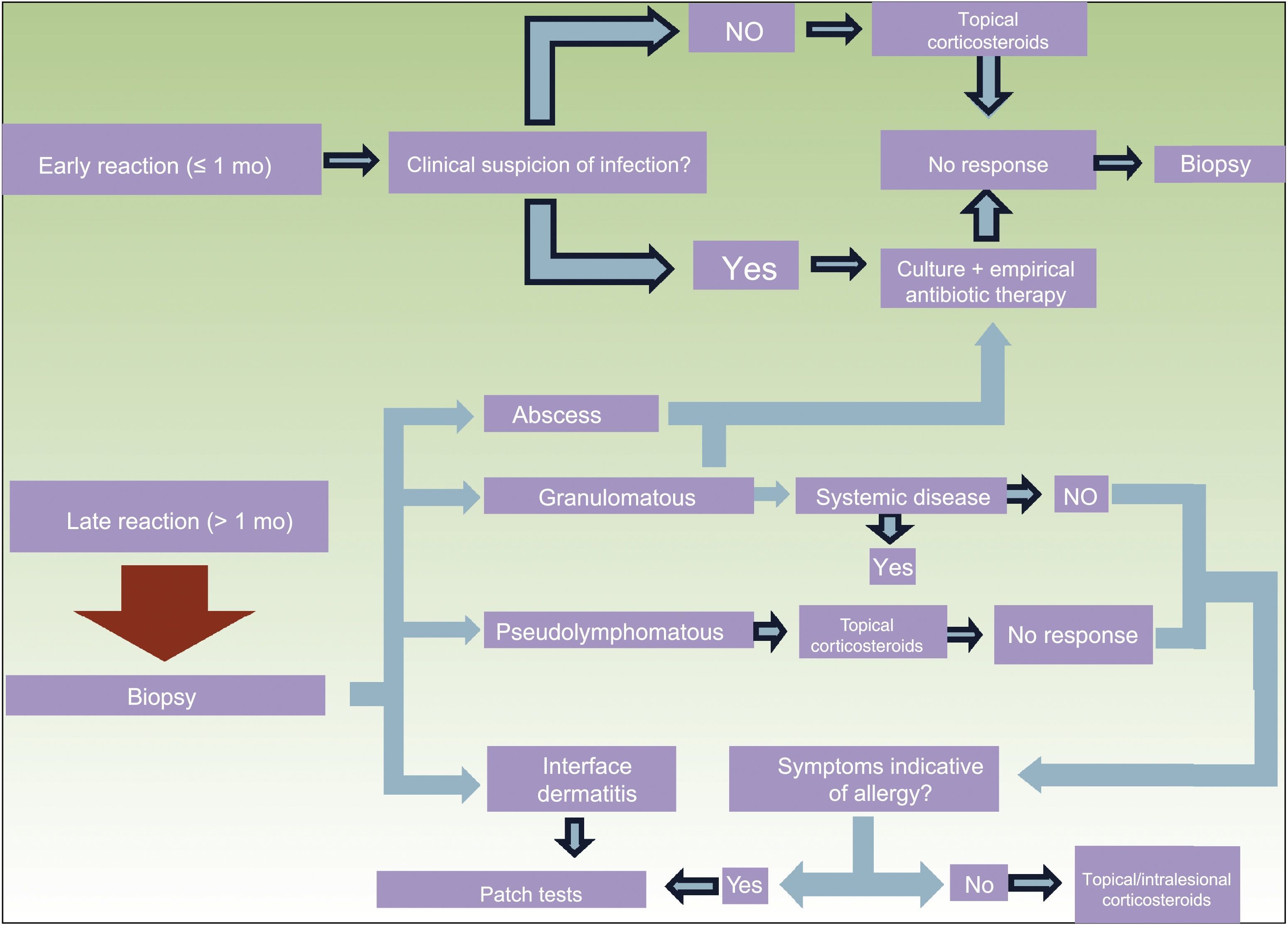
DiscussionTattooing often exposes the skin to foreign bodies that can potentially induce a response.7 We can classify reactions as early (occurring within the first month after the tattoo) and late (occurring more than 1 month after the tattoo). We propose a diagnostic algorithm based on this classification and on our clinical experience (Fig. 4).

The most frequent early complications are transient inflammatory reactions caused by the injury resulting from injection of ink into the skin. These usually occur during the first weeks after the tattoo is placed and do not generally require medical or dermatological attention, since tattooists themselves manage them. However, a potential infectious origin should be borne in mind in the case of an early reaction. Infection by microorganisms can occur through contact with nonsterile material, performance of the procedure under unsanitary conditions, and the use of contaminated ink or water. A recent study showed that 10% of marketed inks are contaminated with pathogenic bacteria and that there are no regulations to guarantee the sterility of ink in Spain.8 Clinical manifestations indicative of infection include pain, increased local temperature, suppuration, and ulceration. In our study, 6 of the patients who were infected through contaminated ink had atypical manifestations, with eczematous plaques (Fig. 5). In many cases, the histopathology findings were compatible with foreign body granuloma; abscess or abundant inflammatory infiltrate of polynuclear cells was observed in 3 cases, despite being an expected finding. We obtained negative cultures in 3 of the patients who had been tattooed with ink from the contaminated batch. This finding can be explained by the fact that people who have a tattoo are generally young and in good health, with sufficient immunity to protect them against the microorganisms involved.9,10

Therefore, in any patient who presents with an early reaction in the area of the tattoo, we believe it is essential to culture the purulent secretion and start empiric antibiotic therapy if the reaction is clinically indicative of infection. If the patient's progress is poor, a biopsy will be necessary for the histopathology and microbiology workup (culture for bacteria and mycobacteria). It would be interesting to perform culture to rule out contamination if a sample of the ink used is available. If the patient presents an early reaction, with no signs of infection, we recommend starting treatment with topical corticosteroids. If the reaction is refractory to treatment, we recommended performing a biopsy.
Late complications are those that develop months or even years after the tattoo. A biopsy is essential in all such cases to rule out infections with late manifestations or even systemic infections. Furthermore, it would help us to make a diagnosis based on histologic patterns.
According to the literature, the presence of noninfectious granulomas is uncommon; however, in our series, this pattern was observed in 2 patients, probably because the particles of pigment that are deposited in the dermis are identified as microscopic foreign bodies.11–13 Such a reaction should lead us to rule out systemic granulomatous disease. Patch testing should be ordered in cases where the symptoms point to an allergic reaction.
The pseudolymphomatous pattern is characterized by a dense lymphocytic infiltrate, which was shown to be polyclonal in the immunohistochemical evaluation. The cause of this type of immune response is unknown, although chronic antigenic stimulation is thought to be responsible.13,14 We propose starting treatment with topical corticosteroids for such reactions. If the lesion persists and clinical manifestations compatible with an allergic reaction appear, we should consider using patch tests.
Lichenoid interface dermatitis was the most frequent histologic pattern in the late reactions and was associated with allergic reactions. This inflammatory infiltrate of the papillary dermis and basal layer of the epidermis is composed of mononuclear cells and macrophages loaded with intracellular pigment. Eosinophils are not a constant finding.14 In our experience, this histologic pattern was the most frequent in cases of probable allergic reaction. Allergic reactions to ink are not common. Their onset is usually late, since they normally result from primary sensitization. Once initiated, the reaction is permanent and does not usually respond to topical corticosteroids. Three clinical patterns that point to allergic reaction to ink were recently reported, although they are not specific. The 3 patterns are plaque-like, hyperkeratotic, and ulcerative-necrotic.5 In the sample we report, we were able to show a different pattern that also points to allergic contact dermatitis, namely, a lichenoid-papular pattern involving nonconfluent pruriginous papules arranged homogeneously on specific areas of color in the tattoo but that do not affect the other colors (Fig. 6). In the present series, the eczematous plaque pattern was the most common, although the lichenoid-papular pattern was also observed in 3 patients, probably because the pigment is injected into the dermis and does not come into direct contact with the epidermis; therefore, the clinical and histologic reaction may differ from the typical manifestations of contact dermatitis. We propose that both clinical patterns point to an allergic reaction. Furthermore, the lesions are usually monomorphic and uniform, affecting all the areas tattooed with the problem color. Patch tests are sometimes ordered for patients with a late reaction that does not affect the whole area tattooed with the problem color; therefore, by definition, the reaction is not an allergic reaction to ink and the yield of the tests is zero. The appearance of identical skin manifestations in areas of the same color on previous tattoos supports an allergic reaction. We observed this phenomenon in a patient with allergic contact dermatitis to red ink, which, according to data from the literature, is the color that most frequently causes allergic reactions. In our experience, there are no differences between reactions to red ink and reactions to black ink, probably because black tattoos are more frequent.

When a patient with a suspected allergic reaction to a tattoo is assessed, most skin allergy units apply their national standard series, a specific metal series, and a textile colorant series, as well as the problem ink. The standard metal series is used because inks can contain pigments manufactured from inorganic metal salts. However, metal salts are being replaced by organic molecules, such as azo pigments and quinacridones.15–17 The specific battery for textile colorants includes several pigments, although we cannot be certain that it contains those used in the tattooed patient. The usefulness of patch tests in this context is not completely clear. In most cases the result is negative or inconsistent, and cases with positive results and an appropriate clinical correlation are exceptional.18 This lack of sensitivity and specificity of patch tests generates several hypotheses. Some authors propose that negative results could be attributed to poor penetration of the skin by the ink used in the tests. Others state that the real allergen is not present in its native form in inks and believe that these are formed in the dermis after a haptenization process. Sunlight could play a role in the process, thus explaining photosensitivity in reactions to tattoos.18–21
Despite the data reported above, we believe that patch testing should be used in all patients with a late reaction to a tattoo, compatible symptoms, and biopsy-proven lichenoid interface dermatitis. In such cases, only the ink and the standard series should be used, since neither the metal series nor the textile series has proven useful.18 Conceptually, intradermal tests would be more specific for the assessment of these patients, although they are not without risks and their use is not ethical.22–24 We hope that in the future, more information on the composition of the inks will enable us to perform patch testing to detect allergens with greater accuracy and thus demonstrate the compound responsible for allergic contact dermatitis.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: González-Villanueva I, Silvestre Salvador J. ¿Qué procedimientos diagnósticos deberíamos realizar ante una sospecha de reacción alérgica a un tatuaje? Propuesta basada en nuestra casuística. Actas Dermosifiliogr. 2018;109:162–172.



