

Omalizumab is a recombinant humanized monoclonal antibody that inhibits immunoglobulin E. It has been approved for the treatment of severe asthma and chronic spontaneous urticaria refractory to other treatments. Its use in the management of chronic inducible urticaria (a type triggered by certain stimuli) is still considered off-label, although this use has been discussed in some consensus papers. This review brings together case reports and case series describing the use of omalizumab to treat chronic inducible urticaria. We analyze the most important aspects of the cases and the outcomes reported. The results seem to position omalizumab as a potentially effective, safe treatment alternative in some cases of chronic inducible urticaria.
Omalizumab es un anticuerpo monoclonal recombinante humanizado anti-IgE actualmente aprobado para el tratamiento del asma grave y de la urticaria crónica espontánea refractarios a otros tratamientos. Su empleo en el manejo de las urticarias crónicas inducibles (aquellas que se desencadenan ante determinados estímulos), si bien está contemplado en algunas guías de consenso, sigue siendo un uso «fuera de indicación». El objetivo de esta revisión es reunir los casos y series de casos publicados de este tipo de urticarias tratadas con omalizumab, analizando las características más relevantes y los resultados terapéuticos. Los resultados parecen posicionar a omalizumab como una potencial alternativa eficaz y segura en el tratamiento de algunos casos de urticaria crónica inducible.
Omalizumab is a recombinant humanized anti-immunoglobulin (Ig) E monoclonal antibody. By binding to IgE at the site that interacts with the receptors on target cells, this drug reduces the levels of free IgE in plasma, resulting in a reduction of the number of high-affinity IgE receptors on basophils and mast cells.1,2
Initially approved for treating moderate to severe asthma, omalizumab was approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of chronic spontaneous urticaria (CSU) in 2014. The current consensus-based guidelines of the European Academy of Allergology and Clinical Immunology, the Global Allergy and Asthma European Network, the European Dermatology Forum, and the World Allergy Organization classify omalizumab as a third-line treatment for chronic urticaria refractory to high-dose antihistamine therapy.3
Omalizumab has proven highly effective in treating CSU, and its safety profile is good. The most severe adverse effect, an anaphylactic reaction, has been reported only rarely in postapproval vigilance systems established to reduce risk.1,4
Omalizumab for the treatment of inducible chronic urticaria (InCU), which develops in response to certain stimuli, usually physical ones, continues to be an off-label use, but case reports referring to this alternative therapy are increasing in number. The various types of InCU are listed in Table 1.
We reviewed the published cases of omalizumab-treated InCU, analyzing clinical characteristics and outcomes. Each InCU subtype was analyzed separately. Case reports were found in MEDLINE through PubMed, using the ClinicalKey search engine. We also searched for clinical trials in ClinicalTrials.gov.
Chronic Cold UrticariaChronic cold urticaria appears after the skin is exposed to low temperatures and can also appear in response to eating cold food.5 This form accounts for about 3% of CSU cases.6
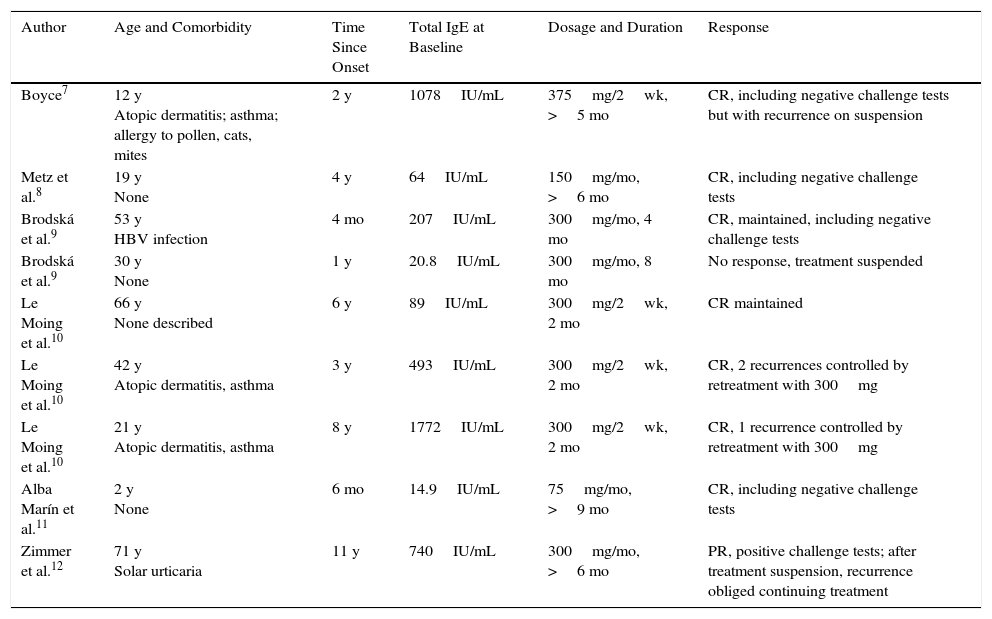
Table 2 lists 9 cases of cold urticaria treated with omalizumab. In addition, the case series by Metz et al.13 and Sussman et al.14 described 5 and 6 more cases, respectively, bringing the total to 20. Those series only provided us with data related to treatment characteristics and outcomes, although more information was available for some cases that had been previously reported individually.
Cases of Chronic Cold Urticaria Treated With Omalizumab.
| Author | Age and Comorbidity | Time Since Onset | Total IgE at Baseline | Dosage and Duration | Response |
|---|---|---|---|---|---|
| Boyce7 | 12 y Atopic dermatitis; asthma; allergy to pollen, cats, mites | 2 y | 1078IU/mL | 375mg/2wk, >5 mo | CR, including negative challenge tests but with recurrence on suspension |
| Metz et al.8 | 19 y None | 4 y | 64IU/mL | 150mg/mo, >6 mo | CR, including negative challenge tests |
| Brodská et al.9 | 53 y HBV infection | 4 mo | 207IU/mL | 300mg/mo, 4 mo | CR, maintained, including negative challenge tests |
| Brodská et al.9 | 30 y None | 1 y | 20.8IU/mL | 300mg/mo, 8 mo | No response, treatment suspended |
| Le Moing et al.10 | 66 y None described | 6 y | 89IU/mL | 300mg/2wk, 2 mo | CR maintained |
| Le Moing et al.10 | 42 y Atopic dermatitis, asthma | 3 y | 493IU/mL | 300mg/2wk, 2 mo | CR, 2 recurrences controlled by retreatment with 300mg |
| Le Moing et al.10 | 21 y Atopic dermatitis, asthma | 8 y | 1772IU/mL | 300mg/2wk, 2 mo | CR, 1 recurrence controlled by retreatment with 300mg |
| Alba Marín et al.11 | 2 y None | 6 mo | 14.9IU/mL | 75mg/mo, >9 mo | CR, including negative challenge tests |
| Zimmer et al.12 | 71 y Solar urticaria | 11 y | 740IU/mL | 300mg/mo, >6 mo | PR, positive challenge tests; after treatment suspension, recurrence obliged continuing treatment |
Abbreviations: CR, complete response; HBV, hepatitis B virus; Ig, immunoglobulin; PR, partial response.
The most frequent comorbidities recorded, asthma and atopy (Table 2), showed no apparent associated variations in response to treatment. Similarly, pretreatment IgE levels were variable and lacked a clear correlation with response. Omalizumab doses ranged from 75mg/mo in 1 pediatric patient to 375mg/2 wk. Seven out of 9 patients (78%) showed complete response and resolution of symptoms. Recurrence after treatment stopped was approached in 2 ways: by administering occasional additional doses or by reinstating the previous therapeutic regimen. Symptoms resolved with both approaches. In a case reported by Zimmer et al.12 the patient had 2 types of InCU: cold urticaria and solar urticaria. Only partial control of both types was achieved in this patient, although treatment led to significant improvement in quality of life.
Metz et al.13 analyzed a series of 6 cases that included one of the patients included in the Table 8; they found that response to omalizumab was complete in 3 patients (50%). Two of them had been treated at a dosage of 150mg/mo, and 1 patient required 150mg/wk to achieve the same effect. Responses were complete in the series of 6 patients described by Sussman et al.14 at dosages of 150mg/mo (4 patients) and 300mg/mo (2 patients).
Omalizumab treatment led to complete response in 15 out of the 20 cases (75%) in total.
No important adverse effects were reported. The patient described by Brodská and Schimd-Grendelmeier9 experienced fatigue and drowsiness. As that patient did not respond, treatment was suspended.
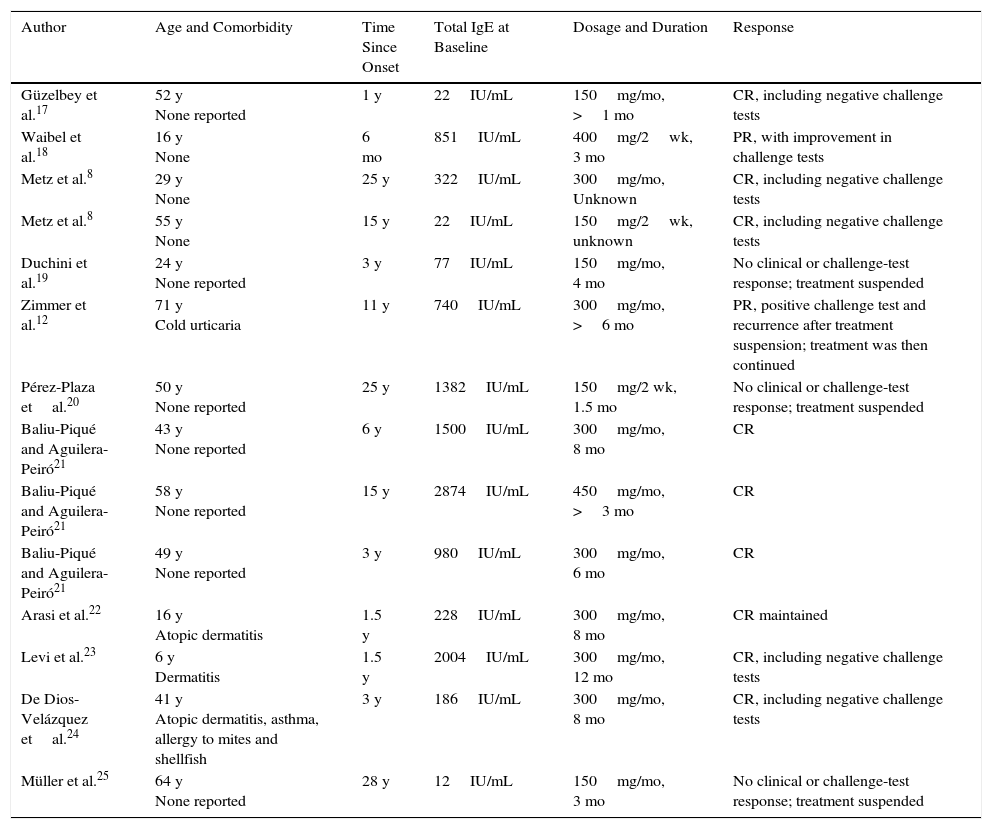
Solar UrticariaSolar urticaria is a rare condition in which wheals appear after exposure to sunlight, visible light, or UV light. Epidemiological data are unavailable because of the low prevalence of this InCU.15,16 Information for the 14 individual reports of patients treated with omalizumab is summarized in Table 3. Two additional patients were included in the series analyzed by Metz et al.,13 but treatment data and response were reported for only one of them.
Solar Urticaria Treated With Omalizumab.
| Author | Age and Comorbidity | Time Since Onset | Total IgE at Baseline | Dosage and Duration | Response |
|---|---|---|---|---|---|
| Güzelbey et al.17 | 52 y None reported | 1 y | 22IU/mL | 150mg/mo, >1 mo | CR, including negative challenge tests |
| Waibel et al.18 | 16 y None | 6 mo | 851IU/mL | 400mg/2wk, 3 mo | PR, with improvement in challenge tests |
| Metz et al.8 | 29 y None | 25 y | 322IU/mL | 300mg/mo, Unknown | CR, including negative challenge tests |
| Metz et al.8 | 55 y None | 15 y | 22IU/mL | 150mg/2wk, unknown | CR, including negative challenge tests |
| Duchini et al.19 | 24 y None reported | 3 y | 77IU/mL | 150mg/mo, 4 mo | No clinical or challenge-test response; treatment suspended |
| Zimmer et al.12 | 71 y Cold urticaria | 11 y | 740IU/mL | 300mg/mo, >6 mo | PR, positive challenge test and recurrence after treatment suspension; treatment was then continued |
| Pérez-Plaza etal.20 | 50 y None reported | 25 y | 1382IU/mL | 150mg/2 wk, 1.5 mo | No clinical or challenge-test response; treatment suspended |
| Baliu-Piqué and Aguilera-Peiró21 | 43 y None reported | 6 y | 1500IU/mL | 300mg/mo, 8 mo | CR |
| Baliu-Piqué and Aguilera-Peiró21 | 58 y None reported | 15 y | 2874IU/mL | 450mg/mo, >3 mo | CR |
| Baliu-Piqué and Aguilera-Peiró21 | 49 y None reported | 3 y | 980IU/mL | 300mg/mo, 6 mo | CR |
| Arasi et al.22 | 16 y Atopic dermatitis | 1.5 y | 228IU/mL | 300mg/mo, 8 mo | CR maintained |
| Levi et al.23 | 6 y Dermatitis | 1.5 y | 2004IU/mL | 300mg/mo, 12 mo | CR, including negative challenge tests |
| De Dios-Velázquez etal.24 | 41 y Atopic dermatitis, asthma, allergy to mites and shellfish | 3 y | 186IU/mL | 300mg/mo, 8 mo | CR, including negative challenge tests |
| Müller et al.25 | 64 y None reported | 28 y | 12IU/mL | 150mg/mo, 3 mo | No clinical or challenge-test response; treatment suspended |
Abbreviations: CR, compete response; Ig, immunoglobulin; PR, partial response.
The most common comorbidity described in the table, as in cases of other types of InCU, was atopy; comorbidity did not appear to be associated with response variations. In contrast, although baseline IgE findings varied, a certain tendency favoring greater response in patients with elevated levels seems to be present: 63% of patients with elevated IgE concentrations (5 out of 8 patients) experienced complete response (Table 3). Dosages ranged from 150 to 800mg/mo. Overall, 9 out of 14 patients (64%) experienced complete response and resolution of symptoms. Eight patients continued treatment. Metz et al.8 reported that symptoms returned on suspension of treatment in 1 patient, but full control of symptoms was again achieved on restarting therapy. Two of the 14 patients (14%) achieved partial response and 3 (21%) showed no response. As mentioned above, the patient described by Zimmer et al.12 was unusual for having 2 types of InCU: both cold and solar urticaria. Partial control of both types was achieved.
One of the 2 additional patients in another series by Metz et al.13 had a complete response and the other had a partial response.
Ten out of 16 patients (62.5%) experienced complete response to omalizumab. No important adverse effects were reported. It is also important to note that treatment was safe in 2 young patients (6 and 16 years of age) at a dosage of 300mg/mo. Both had complete responses. A partial response was reported for a third pediatric patient (16 years of age).
Aubin et al.26 recently published a phase II study in which 10 patients with solar urticaria were treated at a dosage of 300mg/mo for 2 months (3 doses in all). These patients were evaluated through exposure to both artificial light and sunlight (UV-A, UV-B, and the full solar spectrum). The outcome measure was the percentage of patients whose solar urticaria lesions remained under control at week 12 when exposed to UV radiation 10-fold higher than the minimum urticarial dose at baseline. Approximately 40% experienced initial improvement, but efficacy as measured by the main outcome was not statistically significant. However, limitations affecting the study were the lack of a placebo group and the small number of patients enrolled.
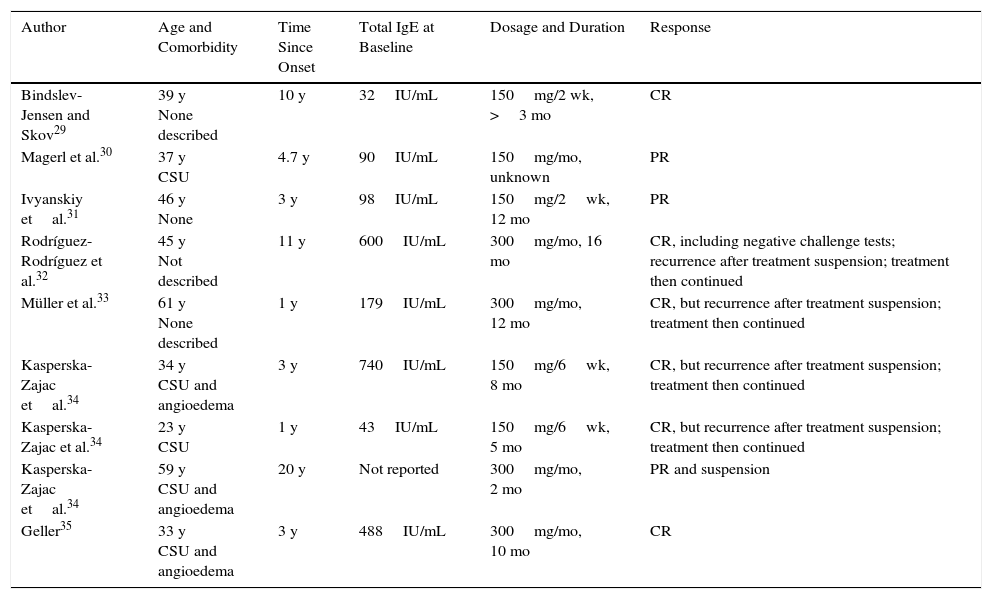
Delayed-Pressure UrticariaThe lesions of delayed-pressure urticaria typically appear 4to 6hours after pressure of varying degrees has been applied to the skin (e.g., as a result of sitting or wearing tight clothing). About 37% of these rare reactions may be associated with CSU, although the lesions may not be noticed because of the delay.27,28 The 9 published cases treated with omalizumab are summarized in Table 4. The series of Metz et al.13 included 8 additional cases, although only partial information was provided.
Delayed-Pressure Urticaria Treated With Omalizumab.
| Author | Age and Comorbidity | Time Since Onset | Total IgE at Baseline | Dosage and Duration | Response |
|---|---|---|---|---|---|
| Bindslev-Jensen and Skov29 | 39 y None described | 10 y | 32IU/mL | 150mg/2 wk, >3 mo | CR |
| Magerl et al.30 | 37 y CSU | 4.7 y | 90IU/mL | 150mg/mo, unknown | PR |
| Ivyanskiy etal.31 | 46 y None | 3 y | 98IU/mL | 150mg/2wk, 12 mo | PR |
| Rodríguez-Rodríguez et al.32 | 45 y Not described | 11 y | 600IU/mL | 300mg/mo, 16 mo | CR, including negative challenge tests; recurrence after treatment suspension; treatment then continued |
| Müller et al.33 | 61 y None described | 1 y | 179IU/mL | 300mg/mo, 12 mo | CR, but recurrence after treatment suspension; treatment then continued |
| Kasperska-Zajac etal.34 | 34 y CSU and angioedema | 3 y | 740IU/mL | 150mg/6wk, 8 mo | CR, but recurrence after treatment suspension; treatment then continued |
| Kasperska-Zajac et al.34 | 23 y CSU | 1 y | 43IU/mL | 150mg/6wk, 5 mo | CR, but recurrence after treatment suspension; treatment then continued |
| Kasperska-Zajac etal.34 | 59 y CSU and angioedema | 20 y | Not reported | 300mg/mo, 2 mo | PR and suspension |
| Geller35 | 33 y CSU and angioedema | 3 y | 488IU/mL | 300mg/mo, 10 mo | CR |
Abbreviations: CR, compete response; CSU, chronic spontaneous urticaria; Ig, immunoglobulin; PR, partial response
The most common comorbidity mentioned in the reports (Table 4) was CSU, present with or without angioedema. The CSU prevalence (55%, in 5 of the 9 patients) was higher than generally reported in the literature but unrelated to response to omalizumab. Baseline IgE levels were highly variable and were once again unrelated to response. Müller et al.33 reported an interesting case of delayed bullous urticaria. The dosages used in these cases, which ranged from 150mg/6 wk to 300mg/mo, were lower than those prescribed for other types of InCU. Two thirds (6 out of 9 patients) showed complete response and resolution of symptoms. Nearly all of them reported full improvement within only 48hours of the first injection. Kasperska-Zajac et al.34 spaced the doses until their patient's symptoms reappeared, applying an optimization strategy made possible because omalizumab acts rapidly.
Seven of the 8 patients (88%) described by Metz et al.13 achieved complete response to therapy, although further details were not provided.
In 13 of the total of 17 published cases (76%) response was complete and in 4 (24%) it was partial. There were no therapeutic failures. Nor were there significant adverse effects.
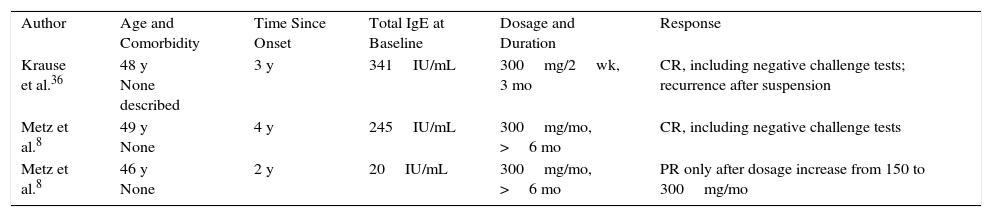
DermographiaDermographia, also known as symptomatic dermographism or urticaria factitia, is a rare InCU in which pruritic wheals are induced by rubbing or scratching the skin.36
Table 5 summarizes the characteristics of the 3 individual case reports in which omalizumab was used. Response was complete in 2 of them (66%). The third had a partial response after the initial dosage was increased. Interestingly, this patient was the only one with a total IgE level that was not elevated at baseline.8 Omalizumab was prescribed at a dosage of 300mg every 2 or 4 weeks. No adverse effects were reported.
Dermographia Treated With Omalizumab.
| Author | Age and Comorbidity | Time Since Onset | Total IgE at Baseline | Dosage and Duration | Response |
| Krause et al.36 | 48 y None described | 3 y | 341IU/mL | 300mg/2wk, 3 mo | CR, including negative challenge tests; recurrence after suspension |
| Metz et al.8 | 49 y None | 4 y | 245IU/mL | 300mg/mo, >6 mo | CR, including negative challenge tests |
| Metz et al.8 | 46 y None | 2 y | 20IU/mL | 300mg/mo, >6 mo | PR only after dosage increase from 150 to 300mg/mo |
Abbreviations: CR, compete response; Ig, immunoglobulin; PR, partial response.
Two patients were described by Metz et al.8 in their first report; their second series described a total of 5 cases of dermographia, 2 of which were the ones reported earlier. All 5 patients achieved complete response to treatment.
In summary, 7 out of 8 of the patients with dermographia (87.5%) had complete responses to omalizumab, 1 patient had a partial response, and there were no therapeutic failures.
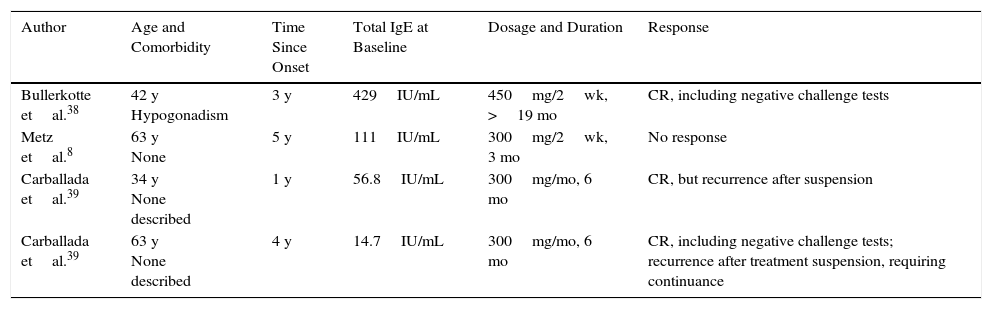
Chronic Heat UrticariaChronic heat urticaria is a rare InCU that is difficult to manage. The reaction is triggered by a local effect of heat from a variety of sources: hot water, hot objects, sunlight (exposed and nonexposed areas), or artificial light.37
Table 6 summarizes the 4 reported cases treated with omalizumab. Three of the 4 patients (75%) achieved complete response. The fourth did not improve except for a slight increase (2°C) in the temperature required for a positive challenge test result.8 In general these patients did not have concurrent diseases of note, with the exception of one who had hypogonadism, which the authors deemed to be of no clinical relevance.38 Response seems to have been unrelated to baseline IgE levels. Dosages ranged from 300mg/mo to 450mg/2 wk. Once again, no important adverse effects were observed.
Chronic Heat Urticaria Treated With Omalizumab.
| Author | Age and Comorbidity | Time Since Onset | Total IgE at Baseline | Dosage and Duration | Response |
|---|---|---|---|---|---|
| Bullerkotte etal.38 | 42 y Hypogonadism | 3 y | 429IU/mL | 450mg/2wk, >19 mo | CR, including negative challenge tests |
| Metz etal.8 | 63 y None | 5 y | 111IU/mL | 300mg/2wk, 3 mo | No response |
| Carballada etal.39 | 34 y None described | 1 y | 56.8IU/mL | 300mg/mo, 6 mo | CR, but recurrence after suspension |
| Carballada etal.39 | 63 y None described | 4 y | 14.7IU/mL | 300mg/mo, 6 mo | CR, including negative challenge tests; recurrence after treatment suspension, requiring continuance |
Abbreviations: CR, compete response; Ig, immunoglobulin.
Vibratory angioedema is one of the least common InCUs. It consists of wheals or angioedema induced by vibrations. Typical triggers are running, motorcycle riding, and using tools such as drills. Playing musical instruments has even been implicated. Only a single case of vibratory angioedema in the literature describes treatment with omalizumab. The patient was a 36-year-old woman whose symptoms had been present for 20 years. She had no concurrent diseases, and her baseline IgE level was 13IU/mL. She showed no clinical improvement after 3 months of treatment with omalizumab (300mg/mo). She did, however, experience a partial response after starting treatment with ketotifen. Improvement was evident in both clinical symptoms and a challenge test (forearm held over a mixer running at increasing speeds). No adverse effects were reported.40
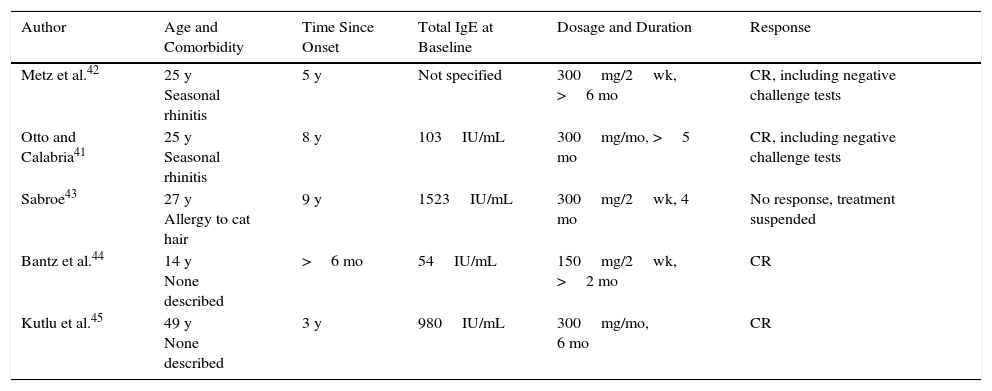
Cholinergic UrticariaCholinergic urticaria is a nonphysical InCU caused by a rise in body temperature. The trigger might be physical exercise, exposure to high ambient temperatures, or emotional stress. Approximately 5% of chronic urticarias are cholinergic.41
Five individual case reports (Table 7) have described omalizumab-treated patients with this form of urticaria. As in other InCUs, the main comorbidity was allergy (seasonal rhinitis or cat allergy) and baseline IgE levels varied considerably. Neither variable appeared to influence the results of treatment. Four of the 5 patients (80%) responded to omalizumab (1 complete response). Treatment failure was reported in 1 case. Dosages were 300mg every 2 or 4 weeks.
Cholinergic Urticaria Treated With Omalizumab.
| Author | Age and Comorbidity | Time Since Onset | Total IgE at Baseline | Dosage and Duration | Response |
|---|---|---|---|---|---|
| Metz et al.42 | 25 y Seasonal rhinitis | 5 y | Not specified | 300mg/2wk, >6 mo | CR, including negative challenge tests |
| Otto and Calabria41 | 25 y Seasonal rhinitis | 8 y | 103IU/mL | 300mg/mo, >5 mo | CR, including negative challenge tests |
| Sabroe43 | 27 y Allergy to cat hair | 9 y | 1523IU/mL | 300mg/2wk, 4 mo | No response, treatment suspended |
| Bantz et al.44 | 14 y None described | >6 mo | 54IU/mL | 150mg/2wk, >2 mo | CR |
| Kutlu et al.45 | 49 y None described | 3 y | 980IU/mL | 300mg/mo, 6 mo | CR |
Abbreviations: CR, compete response.
In the series published by Metz et al.,13 there were 7 additional cases of cholinergic urticaria treated with omalizumab. Four of the patients achieved complete response, 1 responded partially, and 2 experienced no improvement.
In summary, in 8 of the 12 cases (67%) response to omalizumab was complete and there were no adverse effects.
Aquagenic UrticariaAquagenic urticaria is a rare nonphysical InCU. Symptoms appear after exposure to water of any temperature. Water intake does not usually cause symptoms. We were able to find only a single description of an omalizumab-treated patient with this type,46 probably because of the low prevalence of this diagnosis. The patient was a 34-year-old woman with no concurrent diseases who had been experiencing symptoms for 2 years. After 2 months on omalizumab (300mg/4 wk) she experienced complete resolution. Neither circulating IgE levels or adverse effects were reported.46
DiscussionThe indications for omalizumab have broadened in recent years, and this anti-IgE monoclonal antibody was recently approved for treating CSU. Various authors have argued in favor of its therapeutic potential based on the hypothesized role of IgE in the pathogenesis of CSUs or on the effect of IgE on cellular immunity.1,8
At this time, descriptions of omalizumab treatment characteristics and outcomes are only available from case reports and small case series, a situation that presents serious limitations given the possibility of selection bias.
Another basic limitation is the lack of objective outcome criteria that would facilitate consistent analysis of therapeutic effects. In fact, until a short time ago we lacked clinical assessment tools useful for follow-up in InCU. Nothing comparable to scales for CSU in general (the Urticaria Activity Score or the Weekly Urticaria Activity Score) was on hand. After Weller et al.47 described the Urticaria Control Test in a 2014 publication, it underwent cross-cultural adaptation to Castilian Spanish.48 This tool establishes thresholds useful for following patients and monitoring disease control.49,50 However, as such systems were not used when most of the articles we reviewed were written, our analysis of clinical response is necessarily limited.
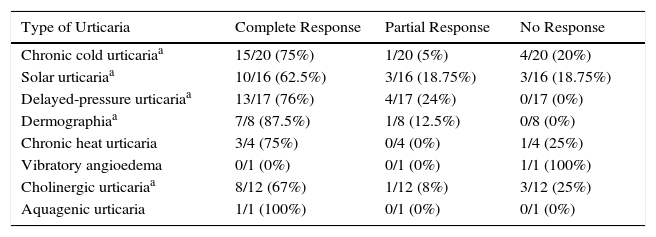
This review, like the case series of Metz et al.,13 found that the patients who seem to benefit the most from treatment with omalizumab are those with dermographia or delayed-pressure urticaria. The complete response rates for these types were 87.5% and 76%, respectively, and there were no reports of treatment failure. The least favorable outcomes were in cases of solar urticaria, where the complete response rate was 62.5%. Response to omalizumab according to different types of InCU are summarized in Table 8.
Response to Omalizumab in Different Varieties of Inducible Chronic Urticaria.
| Type of Urticaria | Complete Response | Partial Response | No Response |
|---|---|---|---|
| Chronic cold urticariaa | 15/20 (75%) | 1/20 (5%) | 4/20 (20%) |
| Solar urticariaa | 10/16 (62.5%) | 3/16 (18.75%) | 3/16 (18.75%) |
| Delayed-pressure urticariaa | 13/17 (76%) | 4/17 (24%) | 0/17 (0%) |
| Dermographiaa | 7/8 (87.5%) | 1/8 (12.5%) | 0/8 (0%) |
| Chronic heat urticaria | 3/4 (75%) | 0/4 (0%) | 1/4 (25%) |
| Vibratory angioedema | 0/1 (0%) | 0/1 (0%) | 1/1 (100%) |
| Cholinergic urticariaa | 8/12 (67%) | 1/12 (8%) | 3/12 (25%) |
| Aquagenic urticaria | 1/1 (100%) | 0/1 (0%) | 0/1 (0%) |
It also appears that baseline IgE levels reported in the publications we reviewed were unrelated to response to omalizumab, in contrast with the pattern seen in asthma. In fact, there were cases of complete response in patients with both normal levels and elevated IgE levels. This observation, emphasized by Metz et al.13 earlier, is consistent with what we have seen in our review. Only in solar urticaria does there seem to be a tendency toward greater efficacy in patients with elevated IgE levels.
The dosages were highly variable in all subtypes of InCU. Regimens sometimes followed recommendations established for asthma (calculated according to IgE level and weight). Sometimes a dosage was prescribed empirically, however, or was based on recommendations for CSU. Francés et al.1 suggested that the optimal dosage probably falls somewhere between 150 and 300mg every 2 to 4 weeks.
At present it is impossible to recommend a treatment duration because of the great variation in the literature and external constraints, given that the reported applications were all off-label. However, based on our review and another retrospective analysis of reported cases of CSU,51 the reintroduction of omalizumab to maintain efficacy in patients who initially responded seems to be safe.
We must emphasize the absence of important adverse effects in any of the published cases. We found only a single case of a patient with cold urticaria who reported fatigue and drowsiness.9
Much more information about the effect of omalizumab on InCU will probably become available in the near future given that several clinical trials are in course. The CUN-OMAL-UCOL,52 CUTEX,53 and UFO54 trials are studying omalizumab for the treatment of cholinergic urticaria, cold urticaria, and dermographia, respectively. In fact, a phase II trial in patients with solar urticaria was recently published,26 as mentioned in the introduction. The publication of such trials may allow us to establish more specific recommendations on indications, dosages, and durations of treatment.
For the moment, omalizumab is positioned as an effective, safe alternative treatment for InCU just as it is for CSU.
Ethical DisclosuresProtection of Human and Animal SubjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of DataThe authors declare that no private patient data are disclosed in this article.
Right to Privacy and Informed ConsentThe authors declare that no private patient data are disclosed in this article.
Conflicts of InterestDrs Chicharro and Rodríguez declare that they have no conflicts of interest. Dr de Argila has served as a clinical advisor for Novartis and has participated in trials sponsored by that laboratory.
Please cite this article as: Chicharro P, Rodríguez P, de Argila D. Omalizumab en el tratamiento de la urticaria crónica inducible. Actas Dermosifiliogr. 2017;108:423–431.



