



The clinical diagnosis of painful nodules is difficult owing to the absence of specific clinical characteristics and the large number of differential diagnoses.1 High-resolution Doppler ultrasound (HRDU) is a very valuable tool for the diagnosis and follow-up of multiple neoplastic, vascular, and inflammatory skin diseases.2
We report the case of a young patient with a painful nodule on the trunk in which HRDU proved useful for evaluation and differential diagnosis.
Case DescriptionA 35-year-old man with no relevant medical history consulted for a painful lesion on the left hemithorax that had first appeared 4 months earlier. The lesion grew slowly, and the pain increased over the last 2 months.
Physical examination revealed a poorly defined and slightly bluish area on the left hemithorax located anteriorly to the axillary midline and a small, soft, mobile, and tender nodule that was difficult to palpate. Dermatoscopy revealed a central blue-violaceous area surrounded by an erythematous halo (Fig. 1A).
: central blue-violaceous area surrounded by an erythematous halo. B, Well-differentiated polylobulated tumor in the dermis (hematoxylin-eosin, original magnification×2). C, The tumor is composed of a biphasic epithelial proliferation comprising small cells arranged around cells with more abundant and clearer cytoplasm that forms ductal structures. No atypia or mitosis is visible (hematoxylin-eosin, original magnification×20).")
A, Dermatoscopy (DermLite II Pro HR, 3Gen): central blue-violaceous area surrounded by an erythematous halo. B, Well-differentiated polylobulated tumor in the dermis (hematoxylin-eosin, original magnification×2). C, The tumor is composed of a biphasic epithelial proliferation comprising small cells arranged around cells with more abundant and clearer cytoplasm that forms ductal structures. No atypia or mitosis is visible (hematoxylin-eosin, original magnification×20).
HRDU with a 22-MHz probe (MyLab Class C, Esaote) revealed a well-defined anechoic image in the dermis and hypodermis. The image was round in the longitudinal plane and polylobulated in the transverse plane. It was 4.2mm thick and had an internal septum measuring 11.9mm on the transverse axis and 5.9mm on its longitudinal axis. Posterior enhancement was observed. Power Doppler mode revealed sparse intralesional vascularization, with low-flow venous and arterial vessels measuring 0.2 to 0.4mm in diameter; spectral Doppler mode revealed that the arterial vessels had a maximum systolic peak of 2.2cm/s (Fig. 2). The ultrasound characteristics led us to suspect a benign subcutaneous tumor or hematoma. However, given the time since onset and the patient's symptoms, the tumor margins were determined using ultrasound, and the lesion was surgically removed.
 reveals a well-defined polylobulated anechoic image with an internal septum located in the dermis and hypodermis. Positive enhancement was observed. The image measured 11.9mm along its transverse axis (A) and 5.9mm along its longitudinal axis (B). Power Doppler revealed sparse intralesional vascularization with arterial and venous vessels measuring between 0.2 and 0.4mm in diameter (C). Spectral Doppler showed that the arterial vessels had a maximum systolic peak of 2.2cm/s (D).")
High-resolution ultrasound with a 22-MHz probe (MyLab class C, Esaote) reveals a well-defined polylobulated anechoic image with an internal septum located in the dermis and hypodermis. Positive enhancement was observed. The image measured 11.9mm along its transverse axis (A) and 5.9mm along its longitudinal axis (B). Power Doppler revealed sparse intralesional vascularization with arterial and venous vessels measuring between 0.2 and 0.4mm in diameter (C). Spectral Doppler showed that the arterial vessels had a maximum systolic peak of 2.2cm/s (D).
Histology revealed a well-defined densely cellular tumor in the dermis composed of 2 cell types: small and intensely basophilic cells arranged around other large, pale cells that clustered to form ductal structures (Figs. 1B and C). These findings were compatible with a diagnosis of eccrine spiradenoma.
DiscussionEccrine spiradenoma is an uncommon, generally benign tumor that originates in the eccrine sweat glands. It generally presents on the trunk of young adults as a single tumor that tends to be painful. The skin may take on a bluish or erythematous tone, as in the present case. Histologically, the tumor is characterized by well-defined nodules with intense cellularity and 2 cell populations: an external population comprising small cells with hyperchromatic nuclei, and an internal population comprising large, pale cells.3
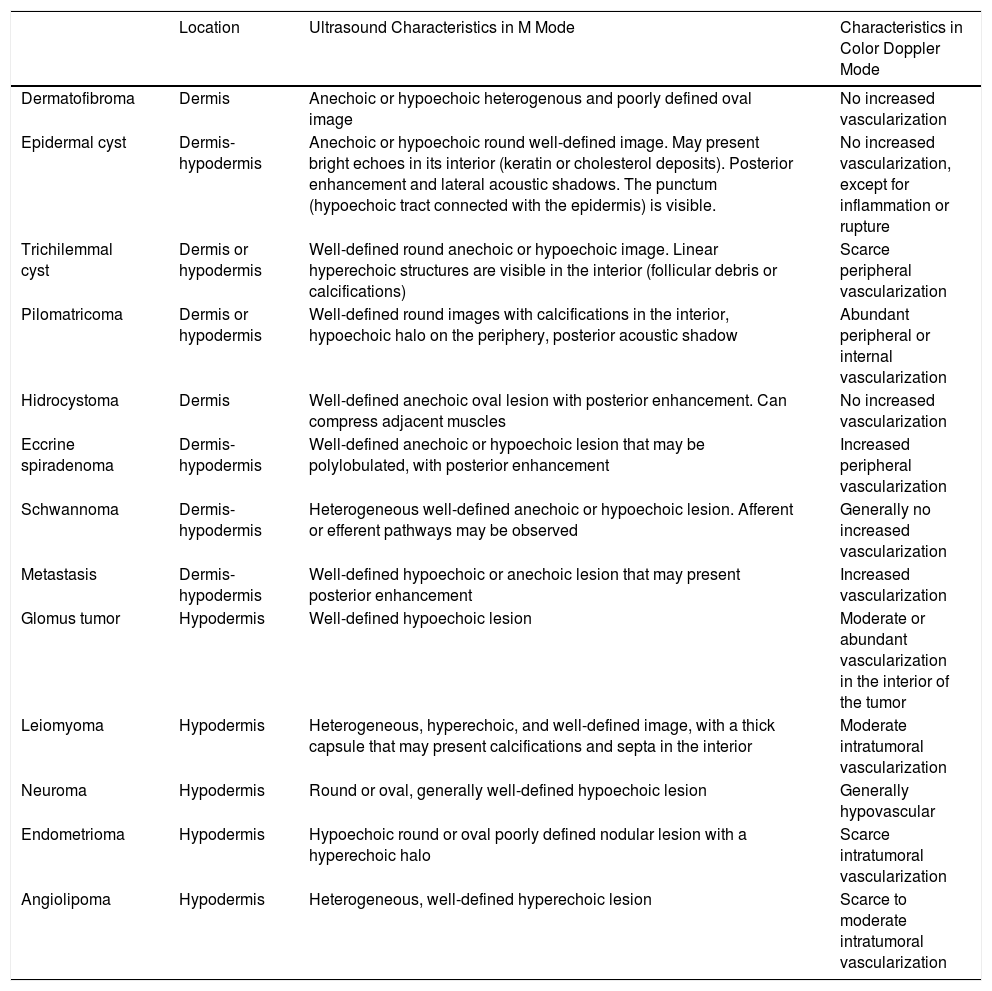
The differential diagnosis of eccrine spiradenoma is very broad and includes inflammatory dermatosis, tumor, and metastasis.1 HRDU can be of value in diagnosis. In the few studies where eccrine spiradenoma has been assessed with ultrasound, the tumor is described as a well-defined hypoechoic or anechoic lobulated image in the dermis or hypodermis, with variable vascular flow and generally peripheral vascularization.3–5 Its location in the dermis-hypodermis enables ultrasound to rule out other painful nodules such as angiolipomas, neurofibromas, neuromas, schwannomas, glomus tumor, endometriomas, and leiomiomas,1 which are generally found in subcutaneous cellular tissue (Table 1).2,6–8 The ultrasound-based differential diagnosis should be performed with potentially painful lesions in the dermis-hypodermis such as epidermal cysts, trichilemmal cysts, pilomatricoma, dermatofibroma, hidrocystoma, and schwannoma, without forgetting cutaneous metastases (Table 1).2,6 It is essential to assess the vascularization of the lesion using Doppler mode, which may help to rule out malignancy with high specificity and sensitivity.9
Differential Diagnosis and Ultrasound Characteristics of Painful Dermal-Hypodermal Lesions.
| Location | Ultrasound Characteristics in M Mode | Characteristics in Color Doppler Mode | |
|---|---|---|---|
| Dermatofibroma | Dermis | Anechoic or hypoechoic heterogenous and poorly defined oval image | No increased vascularization |
| Epidermal cyst | Dermis-hypodermis | Anechoic or hypoechoic round well-defined image. May present bright echoes in its interior (keratin or cholesterol deposits). Posterior enhancement and lateral acoustic shadows. The punctum (hypoechoic tract connected with the epidermis) is visible. | No increased vascularization, except for inflammation or rupture |
| Trichilemmal cyst | Dermis or hypodermis | Well-defined round anechoic or hypoechoic image. Linear hyperechoic structures are visible in the interior (follicular debris or calcifications) | Scarce peripheral vascularization |
| Pilomatricoma | Dermis or hypodermis | Well-defined round images with calcifications in the interior, hypoechoic halo on the periphery, posterior acoustic shadow | Abundant peripheral or internal vascularization |
| Hidrocystoma | Dermis | Well-defined anechoic oval lesion with posterior enhancement. Can compress adjacent muscles | No increased vascularization |
| Eccrine spiradenoma | Dermis-hypodermis | Well-defined anechoic or hypoechoic lesion that may be polylobulated, with posterior enhancement | Increased peripheral vascularization |
| Schwannoma | Dermis-hypodermis | Heterogeneous well-defined anechoic or hypoechoic lesion. Afferent or efferent pathways may be observed | Generally no increased vascularization |
| Metastasis | Dermis-hypodermis | Well-defined hypoechoic or anechoic lesion that may present posterior enhancement | Increased vascularization |
| Glomus tumor | Hypodermis | Well-defined hypoechoic lesion | Moderate or abundant vascularization in the interior of the tumor |
| Leiomyoma | Hypodermis | Heterogeneous, hyperechoic, and well-defined image, with a thick capsule that may present calcifications and septa in the interior | Moderate intratumoral vascularization |
| Neuroma | Hypodermis | Round or oval, generally well-defined hypoechoic lesion | Generally hypovascular |
| Endometrioma | Hypodermis | Hypoechoic round or oval poorly defined nodular lesion with a hyperechoic halo | Scarce intratumoral vascularization |
| Angiolipoma | Hypodermis | Heterogeneous, well-defined hyperechoic lesion | Scarce to moderate intratumoral vascularization |
Curiously, despite being a solid tumor, eccrine spiradenoma may appear as a cystic lesion on ultrasound. Preliminary data suggest that various tumors such schwannomas, leiomyomas, dermatofibromas, dermatofibrosarcoma protuberans, histiocytomas, and eccrine spiradenoma, all of which appear as solid tumors in histopathology, may occasionally present anechoic patterns, with posterior enhancement and even absence of flow in color Doppler. They may also be confused with cysts, thus potentially leading to an erroneous diagnosis.5 The incidence of solid tumors with cystic ultrasound characteristics was 5% in a series of 430 cases.5 Lange et al.10 believe that this could be explained by the histological characteristics of the lesion: the more homogeneous and dense the cell population is, the more likely the lesion is to present as homogeneous, well-defined, and hypoechoic, with posterior enhancement.
In the case we report, HRDU enabled us to identify an uncommon tumor, eccrine spiradenoma, which is difficult to diagnose. A broad spectrum of tumors, including eccrine spiradenoma, may present clinically as painful nodules and on ultrasound as cysts or pseudocysts. It is essential to evaluate these lesions in both planes, with and without compression, and to assess vascularization in Doppler mode in order to avoid diagnostic and therapeutic errors.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Morgado-Carrasco D, Gómez S, Alós L, Giavedoni P. Utilidad de la ecografía en el diagnóstico diferencial de un nódulo doloroso en el tórax. Actas Dermosifiliogr. 2018;109:570–573.



