

Malignant melanoma is a highly immunogenic cancer1 and immunosuppression may affect its incidence and outcome. We describe a retrospective case series of 12 adult patients with a diagnosis of melanoma following sold-organ transplant from 1996 to 2017 in the dermatology department. During the study period, we found more than 1650 solid-organ transplant patients in follow-up, most of whom had received a kidney transplant. Twelve cases of melanoma were diagnosed, 8 of which were men and 4, women. The mean age at transplant was 55.5 years (interval, 29-73 y) and the mean age at melanoma diagnosis was 69 years (interval, 45-78 y). The mean time from transplant to diagnosis of melanoma was 8.5 years (interval, 1-22 y). The majority (9 patients) received a kidney transplant, and the most frequent location of the melanoma was the face. Three cases were in situ melanoma and, of the patients with invasive melanoma, the Breslow thickness was 0.65 mm (interval, 0.30-1.24 mm). The mean follow-up time was 6.5 years (interval, 0.12-17 y). Only 1 patient presented recurrence of the disease, with lymph-node infiltration 14 years after the initial diagnosis (Patient 8). No deaths due to melanoma were observed; however, Patient 11 was in an advanced state on diagnosis and died a month-and-a-half after diagnosis of the melanoma, due to a massive acute myocardial infarction, before chemotherapy was instated.
Skin cancer is the most common neoplasia after transplant. Regarding the association between melanoma and transplant, 3 main scenarios should be analyzed:
- -
The first scenario refers to patients with a history of melanoma. These patients should be ruled out as donors, in accordance with the consensus report of the Spanish National Transplant Organization (May 2006) (Table 1).
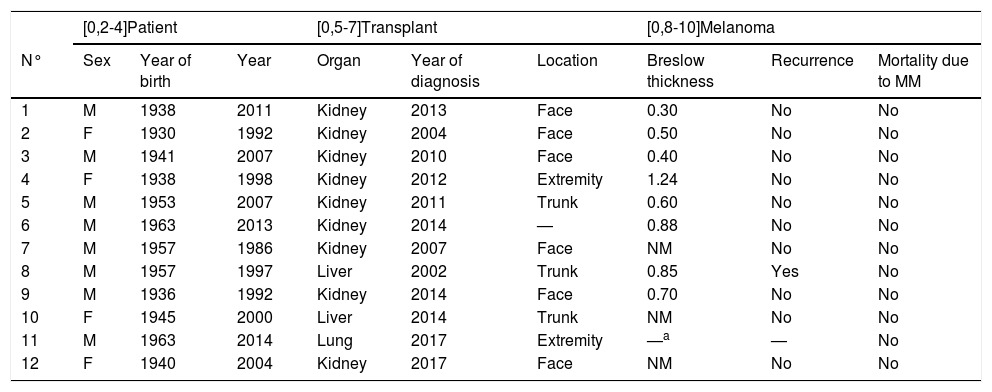
Table 1.Characteristics of Study Patients.
[0,2-4]Patient [0,5-7]Transplant [0,8-10]Melanoma N° Sex Year of birth Year Organ Year of diagnosis Location Breslow thickness Recurrence Mortality due to MM 1 M 1938 2011 Kidney 2013 Face 0.30 No No 2 F 1930 1992 Kidney 2004 Face 0.50 No No 3 M 1941 2007 Kidney 2010 Face 0.40 No No 4 F 1938 1998 Kidney 2012 Extremity 1.24 No No 5 M 1953 2007 Kidney 2011 Trunk 0.60 No No 6 M 1963 2013 Kidney 2014 — 0.88 No No 7 M 1957 1986 Kidney 2007 Face NM No No 8 M 1957 1997 Liver 2002 Trunk 0.85 Yes No 9 M 1936 1992 Kidney 2014 Face 0.70 No No 10 F 1945 2000 Liver 2014 Trunk NM No No 11 M 1963 2014 Lung 2017 Extremity —a — No 12 F 1940 2004 Kidney 2017 Face NM No No MM, malignant melanoma; NM, not measurable because they were in situ melanomas.
- -
The second scenario involves patients with melanoma diagnosed before transplant. To date, no evidence exists to suggest an increase in the risk of recurrence or higher mortality in patients with a history of melanoma prior to transplant.2–4 After reviewing 68 patients with melanoma, who subsequently received a transplant, and comparing them with 141,441 patients with melanoma in the general population, Arron et al3 observed no statistically significant differences in mortality specifically due to melanoma; these data support the current practice of considering patients with a personal history of melanoma as candidates for transplant. Guidelines regarding how to act to select patients with a history of melanoma as transplant recipients are scarce; in 2016, Zwald et al5 proposed the recommendations for action shown in Table 2.
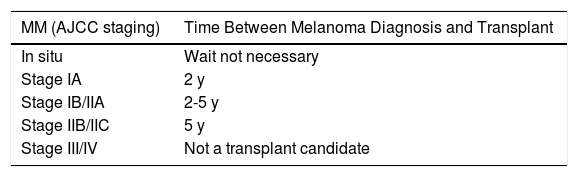
Table 2.Recommended Waiting Times Before Transplant for Patients With a History of Melanoma.
MM (AJCC staging) Time Between Melanoma Diagnosis and Transplant In situ Wait not necessary Stage IA 2 y Stage IB/IIA 2-5 y Stage IIB/IIC 5 y Stage III/IV Not a transplant candidate AJCC, American Joint Committee on Cancer; MM, malignant melanoma.
Source: Zwald et al.5
- -
Finally, in relation to patients in whom melanoma is diagnosed after transplant, an increase in the incidence of melanoma is known to exist in transplant patients. Garret et al studied 10,649 transplant patients and found a melanoma incidence of 125 per 100,000 people/year, compared to between 9 and 18 per 100,000 people/year in the general population. Those authors identified advanced age, Caucasian race, male sex, and having received a thoracic organ as risk factors.6 Ascha et al identified use of sirolimus and cyclosporin as immunosuppressants among the risk factors for melanoma in patients who had undergone a kidney transplant. The mean time between transplant and diagnosis of melanoma was 1.45 years,7 which was less than in our series. The outcome of post-transplant melanoma appears to be determined by the thickness of the tumor on diagnosis and is similar to that of the general population when the Breslow thickness is 1.5 mm or less.4,8 None of our patients presented a Breslow thickness of greater than 1.5 mm. It is important to point out that, although the change from immunosuppressant therapy to mTOR inhibitors is associated with a lower incidence of skin cancer, the antitumor effect of these agents for melanoma alone has only been shown in mouse models.9
In conclusion, in our study, we observed no mortality due to melanoma in patients with post-transplant melanoma, although 1 patient developed a recurrence of the disease and another patient presented metastatic disease at the time of diagnosis. This study is a descriptive, retrospective, observational study and the existence of an association may be fortuitous. We aim to provoke reflection on a circumstance that is rare, but which is of transcendent importance to the life of the patient, as malignant melanoma may be an event that leads to a life change, but denying an organ transplant is a death sentence.
Conflict of interestsThe authors declare that they have no conflict of interest.
The authors would like to thank Elsa Fernández Rubio of the Endocrinology Department and Santiago Rodríguez Tejedor of the Hospital Universitario Cruces Documentation Archive and Management Control Department.
Please cite this article as: Esteban Terradillos S, Gardeazabal García J. Melanoma y trasplante: serie de casos. Actas Dermosifiliogr. 2021;112:193–194.



