




A 39-year-old Bolivian woman with no relevant past medical history presented with multiple asymptomatic lesions on both hands that had first appeared 5 years earlier. No treatment had been applied. The patient reported that a maternal aunt had similar lesions at the same site.
Physical ExaminationPhysical examination revealed numerous yellowish papules from 2 to 4mm in diameter on the palms of both hands (Figs. 1A and 1B), occasionally grouped together forming plaques, as well as isolated lesions on the lateral and dorsal aspects of the fingers.
Histopathology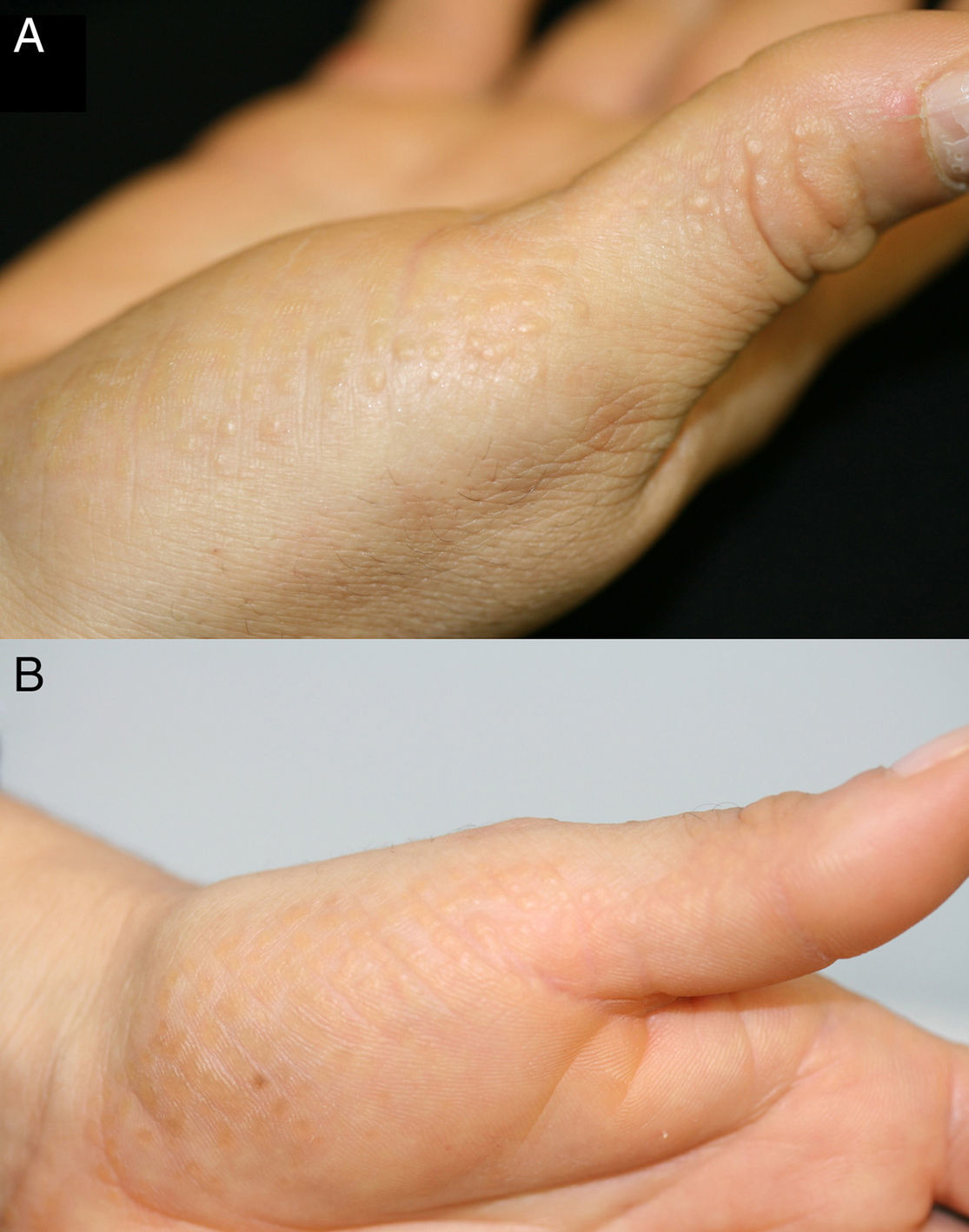
A biopsy specimen was taken from one of the lesions and histologic examination revealed orthokeratotic hyperkeratosis (Fig. 2), with a minimal superficial lymphocytic component in the dermis. The Verhoeff histochemical technique revealed reduction and fragmentation of the reticular fibers (Fig. 3).


What Is Your Diagnosis?
DiagnosisAcrokeratoelastoidosis.
Clinical Course and TreatmentNo treatment was prescribed because the lesions were asymptomatic and the patient was not concerned.
DiscussionAcrokeratoelastoidosis is an idiopathic genodermatosis, first described by Costa1 in 1953, that affects the palms and soles. It is included in the group of marginal acrokeratodermas, which are characterized by papules and plaques in the lateral margins of the hands and feet; acrokeratoelastoidosis is a hereditary subtype of this group of dermatoses.2 Both dominant and recessive patterns of autosomal inheritance have been described.1,3 Acrokeratoelastoidosis is characterized by well-defined skin-colored or yellowish polygonal papules, some umbilicated, from 2 to 5mm in diameter.1 The lesions are located on the transitional margin between the dorsal and palmar skin of the hands or between the dorsal and plantar skin of the feet and are usually asymptomatic, although they can be pruritic or be associated with hyperhidrosis.4 The distribution is variable and the lesions can be found either in isolation or grouped together forming plaques. Onset frequently occurs in young adulthood.1
The etiology and pathogenesis of acrokeratoelastoidosis are unknown. The causal mechanism is suspected to be the anomalous production of bundles of elastic fibers by the fibroblasts, leading to the fragmentation and reduction in quantity of these fibers in the reticular dermis (elastorrhexis).5 Microscopy reveals a decrease in the number of fibroblasts, which contain dense cytoplasmic granules that could be precursors of reticulin.4 In patients affected by this dermatosis, elastorrhexis without epidermal skin changes at sites not clinically affected has also been reported.5
The differential diagnosis should include other marginal acrokeratodermas, especially focal acral hyperkeratosis, degenerative collagenous plaques of the hands, and keratoelastoidosis marginalis.1,2,5 Acrokeratoelastoidosis and focal acral hyperkeratosis both belong to the subgroup of hereditary acrokeratodermas and can be differentiated by their histologic features: acrokeratoelastoidosis is characterized by elastorrhexis, whereas in focal acral hyperkeratosis the elastic fibers are present in normal amounts and with a normal distribution.5 Acquired forms of degenerative collagenous plaques of the hands and keratoelastoidosis marginalis appear in manual laborers with intense actinic damage, a history of chronic sun exposure, and repeated trauma injuries of the hands2,5; these conditions usually affect the medial aspect of the thumb and the lateral aspect of the index finger.6
The various treatments used to date—such as cryotherapy, salicylic acid, methotrexate, dapsone, and oral corticosteroids—have been unsatisfactory.2,5 Only acitretin at a dose of 0.5mg/kg/d has shown some usefulness.2
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Panés-Rodríguez A, Jaka-Moreno A, Montero IA-C, Tuneu-Valls A. Múltiples pápulas en ambas manos. Actas Dermosifiliogr. 2017;108:579–580.



