


Herpes zoster is a relatively common disease worldwide, with a detected lifetime incidence between 10% and 20%. The classic clinical picture is characterized by clusters of papular and vesicular lesions on an erythematous base distributed unilaterally along a single dermatome. This characteristic presentation makes herpes zoster easily recognizable, even by non-dermatologist clinicians of different specialties. Involvement of 2 or more unilateral and contiguous dermatomes is not an uncommon finding in older patients and patients with other risk factors for immunosuppression. However, simultaneous involvement of 2 non-contiguous dermatomes—unilaterally or even bilaterally—is an exceptional finding that can make diagnosis difficult. In the literature, this manifestation has been called herpes zoster duplex.1 Isolated cases of patients with involvement of more than 2 non-contiguous dermatomes have been called herpes zoster multiplex.2
We present 2 cases of herpes zoster duplex and 1 of herpes zoster multiplex diagnosed in our department between 2015 and 2017. The clinical and epidemiological characteristics are shown in Table 1.
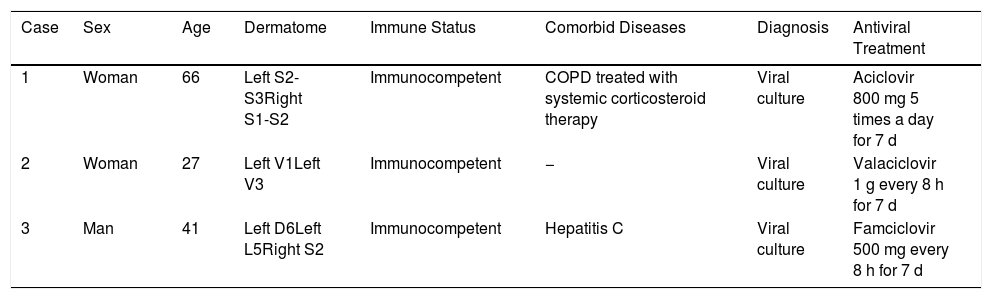
Review of Diagnosed Cases of Herpes Zoster Duplex and Multiplex in the Emergency Department of the Hospital Gregorio Marañón During the Period 2015-2017.
| Case | Sex | Age | Dermatome | Immune Status | Comorbid Diseases | Diagnosis | Antiviral Treatment |
|---|---|---|---|---|---|---|---|
| 1 | Woman | 66 | Left S2-S3Right S1-S2 | Immunocompetent | COPD treated with systemic corticosteroid therapy | Viral culture | Aciclovir 800 mg 5 times a day for 7 d |
| 2 | Woman | 27 | Left V1Left V3 | Immunocompetent | − | Viral culture | Valaciclovir 1 g every 8 h for 7 d |
| 3 | Man | 41 | Left D6Left L5Right S2 | Immunocompetent | Hepatitis C | Viral culture | Famciclovir 500 mg every 8 h for 7 d |
Abbreviations: COPD, chronic obstructive pulmonary disease.
The 2 cases of herpes zoster duplex (cases 1 and 2) occurred in immunocompetent patients aged 27 and 66 years, respectively, who consulted for the acute appearance of unilateral or bilateral vesicular lesions with zosteriform distribution. Neither patient experienced pain in the affected dermatomes or presented fever or other extracutaneous symptoms throughout the process. The patient who presented with herpes zoster multiplex (case 3, Fig. 1), was a male aged 41years who had already started treatment with famciclovir 72h earlier, prescribed by his primary care physician. In spite of this treatment, new lesions continued to appear. None of the 3 patients reported any prior episodes of herpes zoster. In all 3 cases, viral culture of the exudate confirmed the diagnosis a posteriori, with detection of the varicella zoster virus in all 3 cases. The results of serologies performed to rule out HIV infection were negative in all 3 patients. With the diagnosis of herpes zoster duplex in cases 1 and 2 and multiplex in case 3, antiviral treatment was prescribed at standard doses complemented by topical care with zinc sulphate and fusidic acid until the lesions were completely healed.
 as well as D6 (C) on the left side and S2 (D) on the right side.")
The probability of developing herpes zoster duplex or multiplex is extremely low, with a documented incidence in the largest series of less than 0.1% of all herpes zoster cases.3
In 2015, Zhang and Zhou4 reviewed all the cases of herpes zoster duplex reported in the literature, affecting in total 36 patients. They highlighted several associated risk factors in that series: Asian origin (over 66%), older age (44.4% were over 50 years of age), female sex (63.9% were women), and immunosuppression (47.2%) associated with a variety of causes (immunosenescence, HIV, hematologic malignancies, solid organ tumors, chemotherapy, and prolonged therapy with corticosteroids or other immunosuppressive drugs). In a review of the literature published in 1999,2 only 7 cases of herpes zoster multiplex were found, almost all associated with causes of immunosuppression.
Following primary varicella-zoster virus infection, the virus establishes a latent infection in the dorsal and trigeminal root ganglia; this has been demonstrated by viral DNA analysis in autopsies.5 Reactivation of the virus in the ganglion with the highest latent viral load—mediated by multiple triggers—gives rise to the characteristic herpetic lesions in the affected dermatome. In herpes zoster duplex and multiplex, simultaneous reactivation of the virus in different, non-contiguous dorsal ganglia gives rise to the uncharacteristic clinical presentation and is also facilitated by immunosuppression.6 However, other factors that have not yet been elucidated must also play a role because most of the cases reported, including our 3 patients, have occurred in immunocompetent patients.1,3,7–9
In routine clinical practice, classic herpes zoster is usually diagnosed on the basis of the clinical presentation. When there is doubt, however, or when the presentation is atypical, confirmation of the diagnosis by testing is recommended. In our 3 cases, diagnosis was confirmed by viral culture of two cell lines (MRC-5 human lung fibroblasts and A549 human lung tumor epithelial cells). The cultures were maintained for 3 weeks, during which it was checked for cytopathic effect every 3 to 4 days. The appearance of a cytopathic effect was confirmed by staining with monoclonal antiviral antibodies (Argene® Anti Varicella Zoster Virus Ref 11-017), with fluorescence being observed under the microscope in positive cases.
The treatment of patients with herpes zoster duplex and multiplex is the same as that used in classic cases, and involves antiviral coverage, pain control, and topical care. In our patients, follow-up confirmed complete cure without sequelae after the antiviral treatment was completed with the usual dose and treatment duration.
In summary, we consider it important to recognize these rare presentations and their potential association with causes of immunosuppression. In the presence of typical herpetic skin lesions with metameric distribution, the involvement of non-contiguous and/or bilateral dermatomes should not lead us to change the generally accepted treatment regimen, although such cases should be monitored closely.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
We wish to thank Dr. Stavola and Dr. Catalán-Alonso, our colleagues in the Department of Microbiology, for their help in the writing of this article.
Please cite this article as: Rodríguez-Lomba E, Sánchez-Herrero A, Suárez-Fernández R, Pulido-Pérez A. La excepción que confirma la regla: herpes zoster duplex y multiplex. Actas Dermosifiliogr. 2019;110:690–693.



